
Respiratory Pathology — MCQs

On this page
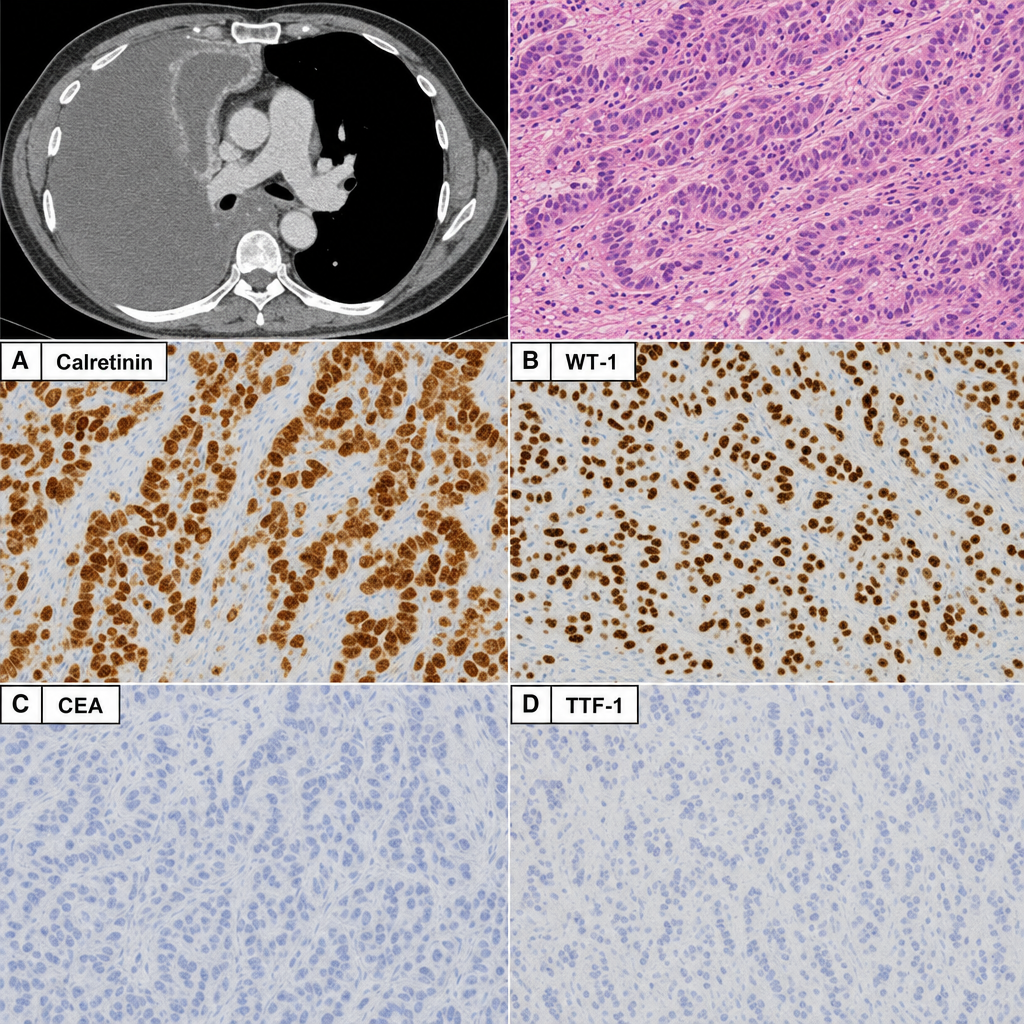
A 60-year-old male with a 30-year history of occupational asbestos exposure presents with progressive dyspnea and massive right-sided pleural effusion. CT scan reveals a circumferential pleural-based mass encasing the right lung. A pleural biopsy is performed. The IHC panel (Image 1) shows: Panel A — strong diffuse nuclear and cytoplasmic positivity for Calretinin in tumor cells; Panel B — strong nuclear positivity for WT-1 in tumor cells; Panel C — negativity for CEA in tumor cells; Panel D — negativity for TTF-1 in tumor cells. Based on this IHC pattern, which of the following best explains why this result is diagnostically significant in distinguishing this lesion from its closest morphological mimic?
A 65-year-old chronic smoker presents with a rapidly enlarging large hilar mass on a chest film associated with significant adenopathy. He also experiences recurrent hypoglycemic spells. Which of the following lung carcinoma subtypes will most commonly lead to this spectrum?
Which of the following is NOT typically seen in ARDS?
A 46-year-old woman presents with fever, hemoptysis, weight loss, and night sweats. She has never smoked and recently returned from a month-long trip to Asia. A chest radiograph reveals apical lesions with cavitation in the left lung. A purified protein derivative (PPD) test is placed, and 48 hours later an 18-mm wheal develops. Sputum cultures reveal numerous acid-fast organisms. This patient is placed on contact precautions, and a regimen for tuberculosis is started. Which of the following disorders does this patient most likely have?
A specimen from a lung biopsy reveals occasional plexiform lesions within pulmonary arterioles. Which of the following conditions is most characteristic of this finding?
Practice by Chapter
Congenital Anomalies
Practice Questions
Atelectasis and Acute Lung Injury
Practice Questions
Obstructive Pulmonary Diseases
Practice Questions
Restrictive Pulmonary Diseases
Practice Questions
Lung Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Lung Tumors
Practice Questions
Pleural Diseases
Practice Questions
Interstitial Lung Diseases
Practice Questions
Occupational Lung Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app