
Reproductive Pathology — MCQs

On this page
Corkscrew shaped endometrial glands are seen in which phase of the menstrual cycle?
Reinke crystalloids can be seen in which of the following sex cord-stromal tumors?
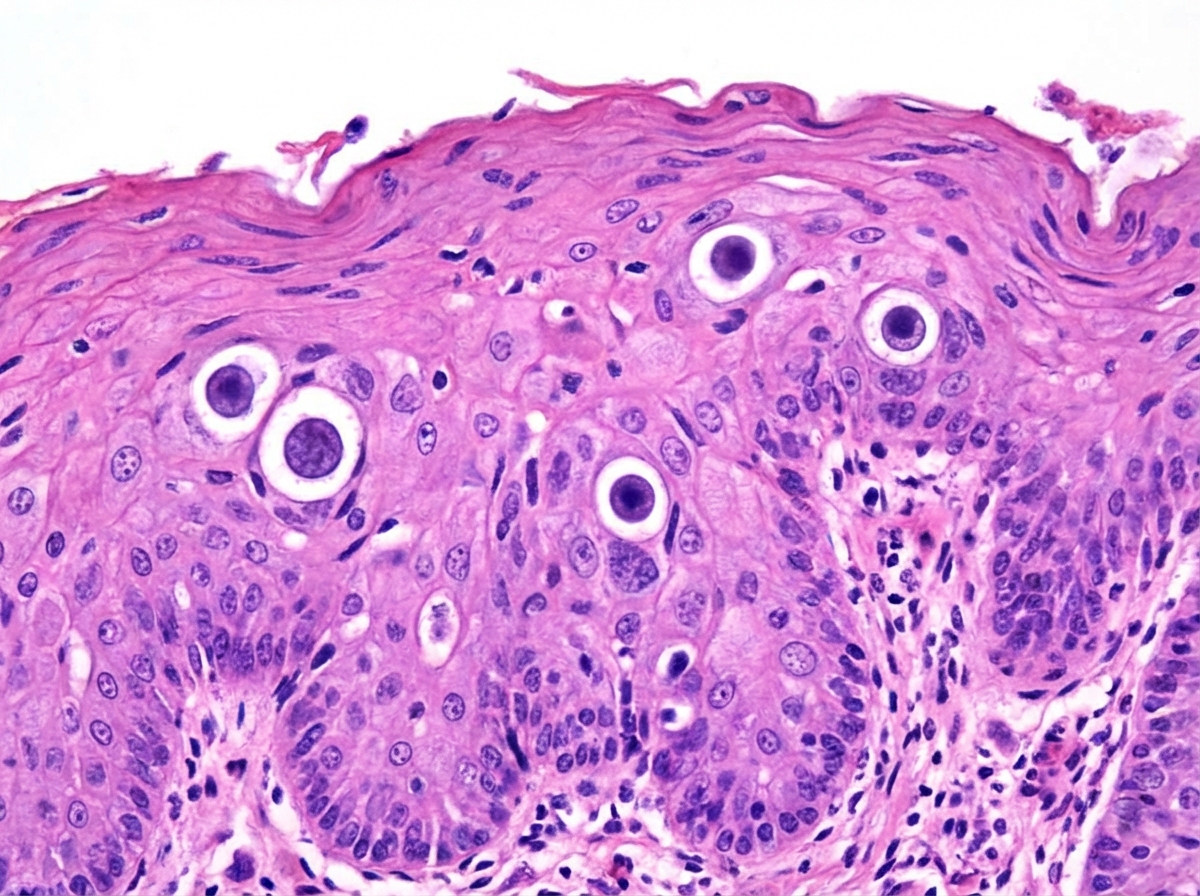
The lesion shown below is caused by:
Type 2 endometrial carcinoma is associated with what histological finding?
Which tumor typically presents with a grape-like cluster appearance and consistency?
A study of patients with postmenopausal uterine bleeding reveals that some of them have malignant neoplasms that arise from prior atypical hyperplastic lesions. The peak incidence is between 55 and 65 years of age in women who have obesity, hypertension, and/or diabetes mellitus. Molecular analysis reveals mutations of the PTEN tumor suppressor gene in most of them. Their malignancies tend to remain localized for years before spreading to local lymphatics. Which of the following neoplasms is most likely to have these characteristics?
Which of the following is NOT true about atrophic testis?
Which of the following markers is NOT typically elevated in a testicular teratoma?
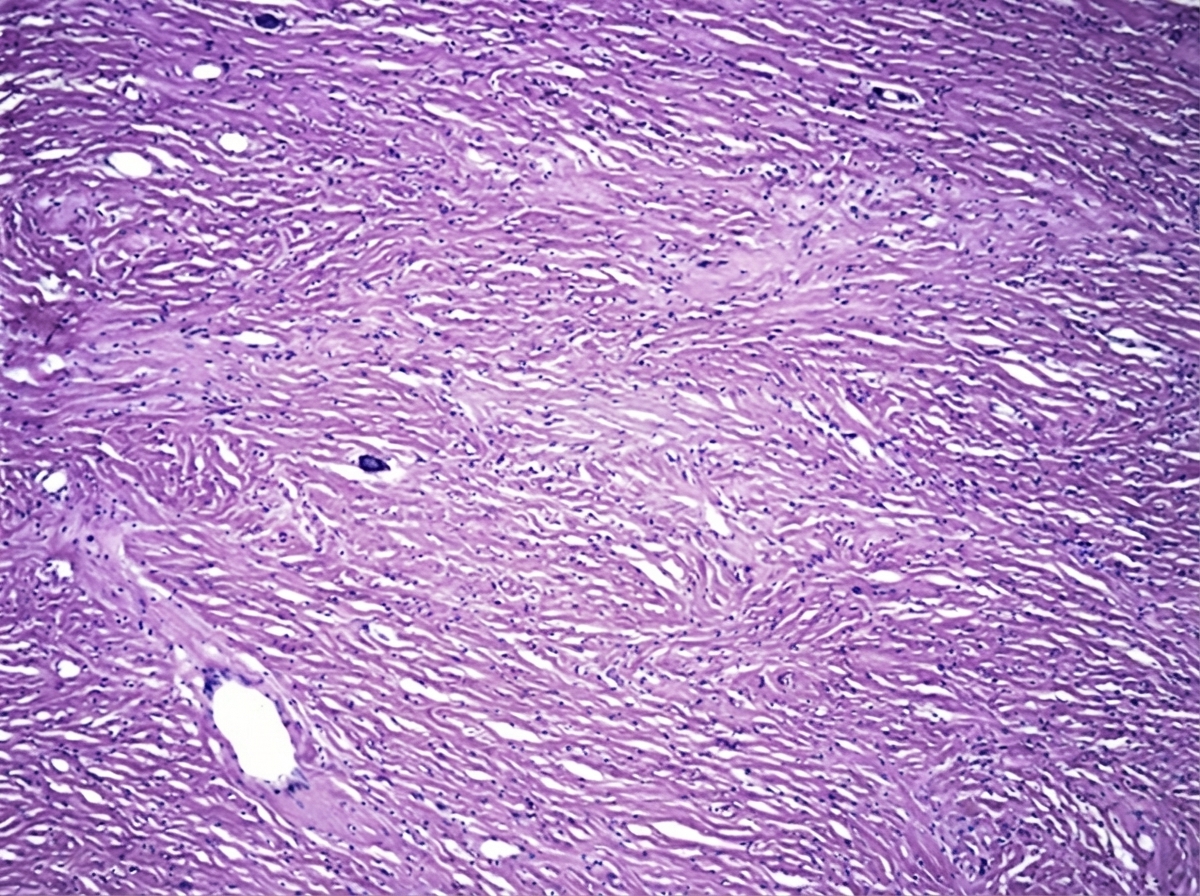
A 35-year-old female underwent hysterectomy, which revealed a well-circumscribed, whorled, white-gray firm nodule on gross examination. What is the most likely diagnosis?
Schiller-Duval bodies are seen in which of the following tumor types?
Practice by Chapter
Diseases of Male Genital Tract
Practice Questions
Testicular Tumors
Practice Questions
Prostate Pathology
Practice Questions
Diseases of Female Genital Tract
Practice Questions
Cervical Pathology and Neoplasia
Practice Questions
Endometrial Pathology
Practice Questions
Ovarian Diseases and Tumors
Practice Questions
Gestational Trophoblastic Disease
Practice Questions
Placental Pathology
Practice Questions
Sexually Transmitted Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app