
Reproductive Pathology — MCQs

On this page
Which of the following histological features characterizes a hydatidiform mole?
A 23-year-old woman presents with a rubbery, freely movable 2-cm mass in the upper outer quadrant of the left breast. A biopsy of this lesion would most likely histologically reveal?
A 25-year-old woman presents with lower abdominal discomfort. The surgical image is given below. What is the most likely diagnosis?
A 30-year-old female presents to the OPD with a 3 cm breast lump in the upper medial quadrant. The lump has an uneven, bosselated surface, and the overlying skin is mildly ulcerated. Microscopic examination reveals the given findings. What is the most likely diagnosis?
A 50 year old female presented with a breast mass that was operated and the microscopic examination in given. What is the diagnosis?
Edematous villi with chromosome XY were found. What will be the diagnosis?
A biopsy from a breast mass in a 55-year-old woman shows infiltrating ductal carcinoma. Immunohistochemistry reveals ER negative, PR negative, and HER2/neu negative. What is the classification of this tumor?
Histopathological features of granulosa cell tumor include all except:
A 30-year-old man presents with a painless testicular mass. An ultrasound shows a well-circumscribed, homogeneous, non-hemorrhagic testicular tumor. Which of the following is the most likely diagnosis?
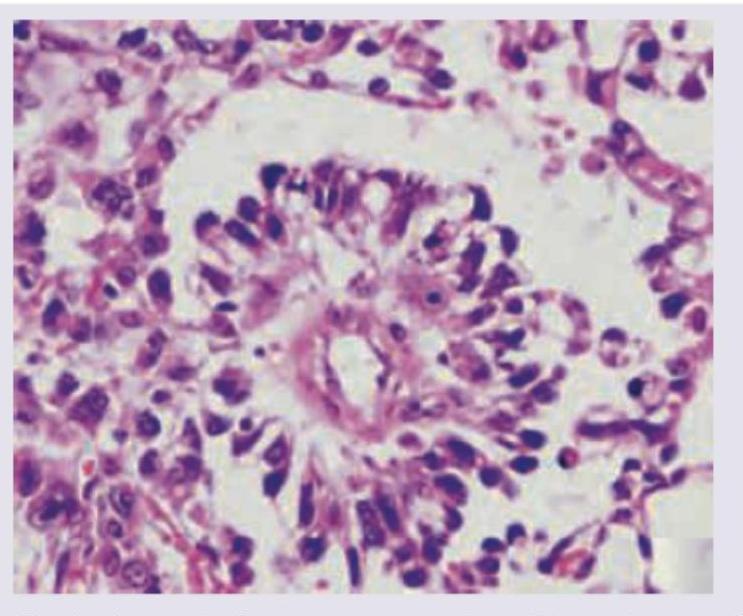
15-year-old girl presents with a big pelvic mass. CT abdomen shows omental thickening and large ovarian mass. The ovarian mass was removed intact during surgical staging, and histopathology showed the following. The specimen findings are diagnostic of?
Practice by Chapter
Diseases of Male Genital Tract
Practice Questions
Testicular Tumors
Practice Questions
Prostate Pathology
Practice Questions
Diseases of Female Genital Tract
Practice Questions
Cervical Pathology and Neoplasia
Practice Questions
Endometrial Pathology
Practice Questions
Ovarian Diseases and Tumors
Practice Questions
Gestational Trophoblastic Disease
Practice Questions
Placental Pathology
Practice Questions
Sexually Transmitted Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app