
Reproductive Pathology — MCQs

On this page
A blighted ovum is characterized by which of the following?
Which of the following is a predisposing factor for carcinoma of the breast?
A 51-year-old woman has noticed an area of swelling with tenderness in her right breast that has worsened over the past 2 months. On physical examination, the 7-cm area of erythematous skin is tender with a rough, firm surface resembling an orange peel. There is swelling of the right breast, nipple retraction, and right axillary non-tender lymphadenopathy. Excisional biopsy of skin and breast is most likely to show which of the following lesions?
What is the most common testicular tumor in the fourth decade of life?
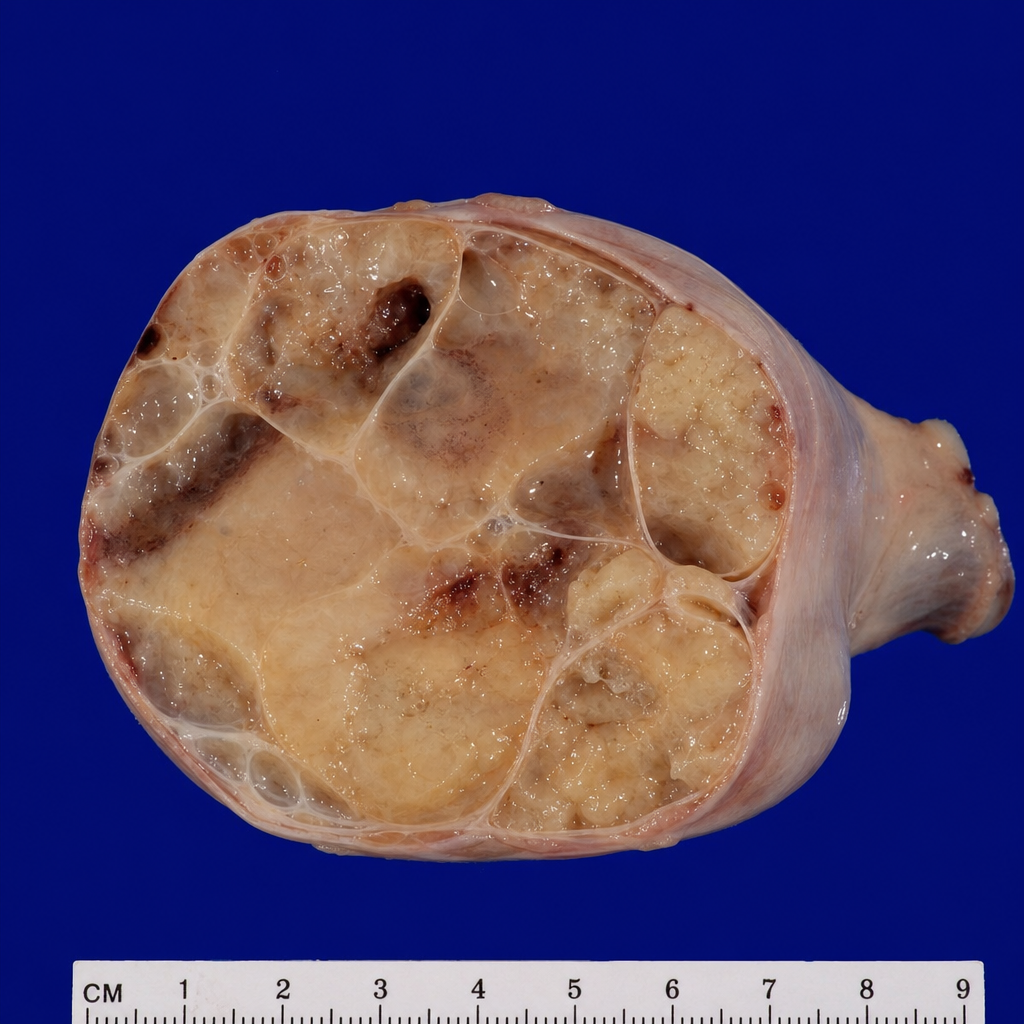
A 20-year-old female presents with a mass in the abdomen. Examination of the removed ovary reveals the specimen shown below. Histology shows large uniform cells with clear cytoplasm, central nuclei, and fibrous septa infiltrated by lymphocytes. Serum LDH is elevated. What is the most probable diagnosis?
A 34-year-old woman has noticed a bloody discharge from the nipple of her left breast for the past 3 days. On physical examination, the skin of the breasts appears normal, and no masses are palpable. There is no axillary lymphadenopathy. She has regular menstrual cycles and is using oral contraceptives. Excisional biopsy is most likely to show which of the following lesions in her left breast?
What is true regarding male breast carcinoma?
Which of the following is NOT a rare histological variant of carcinoma breast with a better prognosis?
A 22-year-old woman nursing her newborn develops a tender erythematous area around the nipple of her left breast. A thick, yellow fluid is observed to drain from an open fissure. Examination of this breast fluid under the light microscope will most likely reveal an abundance of which of the following inflammatory cells?
Which of the following are germ cell tumors of the testis?
Practice by Chapter
Diseases of Male Genital Tract
Practice Questions
Testicular Tumors
Practice Questions
Prostate Pathology
Practice Questions
Diseases of Female Genital Tract
Practice Questions
Cervical Pathology and Neoplasia
Practice Questions
Endometrial Pathology
Practice Questions
Ovarian Diseases and Tumors
Practice Questions
Gestational Trophoblastic Disease
Practice Questions
Placental Pathology
Practice Questions
Sexually Transmitted Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app