
Reproductive Pathology — MCQs

On this page
Which among the following are testicular tumor markers?
Which of the following is associated with Paget's disease of the mammary gland?
A 20-year-old female was diagnosed with granulosa cell tumor of the ovary. Which of the following biomarkers would be most useful for diagnosis and follow-up of the patient?
All of the following are germ cell tumors EXCEPT:
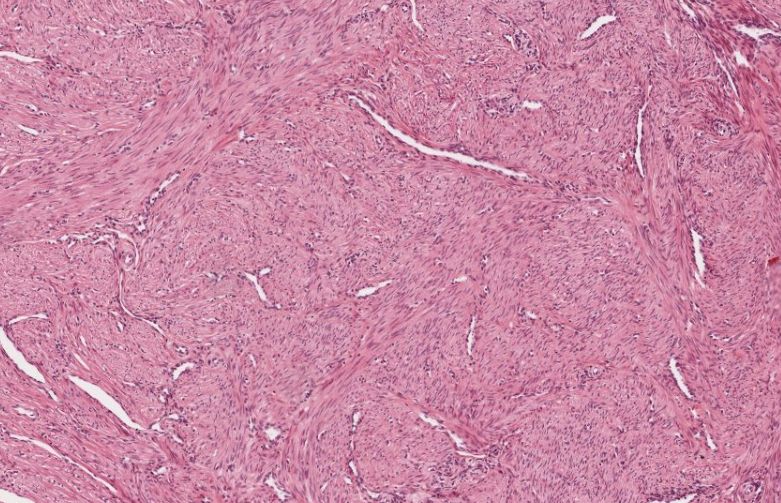
A 45-year-old female underwent hysterectomy for dysfunctional uterine bleeding. The following is a histological finding. Which of the following is the most likely diagnosis?
Which of the following ovarian neoplasms shows Rokitansky's protuberance?
Corpora amylacea are microscopic structures found in which of the following glands?
A patient with a long-standing intrauterine contraceptive device (IUCD) develops chronic pelvic pain. The device is removed, and a biopsy of the endometrium is performed. The biopsy specimen shows a prominent infiltrate composed of lymphocytes, plasma cells, and histiocytes. Which of the following is the most likely diagnosis?
What is the most important prognostic factor in breast carcinoma?
A 49-year-old female presented with postmenopausal bleeding and a uterine cavity growth on sonography. During surgery, the growth is large, multicystic, and exceeds 10 cm in diameter. Granulosa cell tumor is suspected. What characteristic histological finding helps distinguish granulosa cell tumor from other uterine tumors?
Practice by Chapter
Diseases of Male Genital Tract
Practice Questions
Testicular Tumors
Practice Questions
Prostate Pathology
Practice Questions
Diseases of Female Genital Tract
Practice Questions
Cervical Pathology and Neoplasia
Practice Questions
Endometrial Pathology
Practice Questions
Ovarian Diseases and Tumors
Practice Questions
Gestational Trophoblastic Disease
Practice Questions
Placental Pathology
Practice Questions
Sexually Transmitted Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app