
Reproductive Pathology — MCQs

On this page
A 2-year-old boy presents with a palpable mass on his right testicle. After orchiectomy, microscopic examination of the specimen reveals neoplastic cells forming glomeruloid Schiller-Duval bodies. Which serum marker is most useful for monitoring tumor recurrence in this patient?
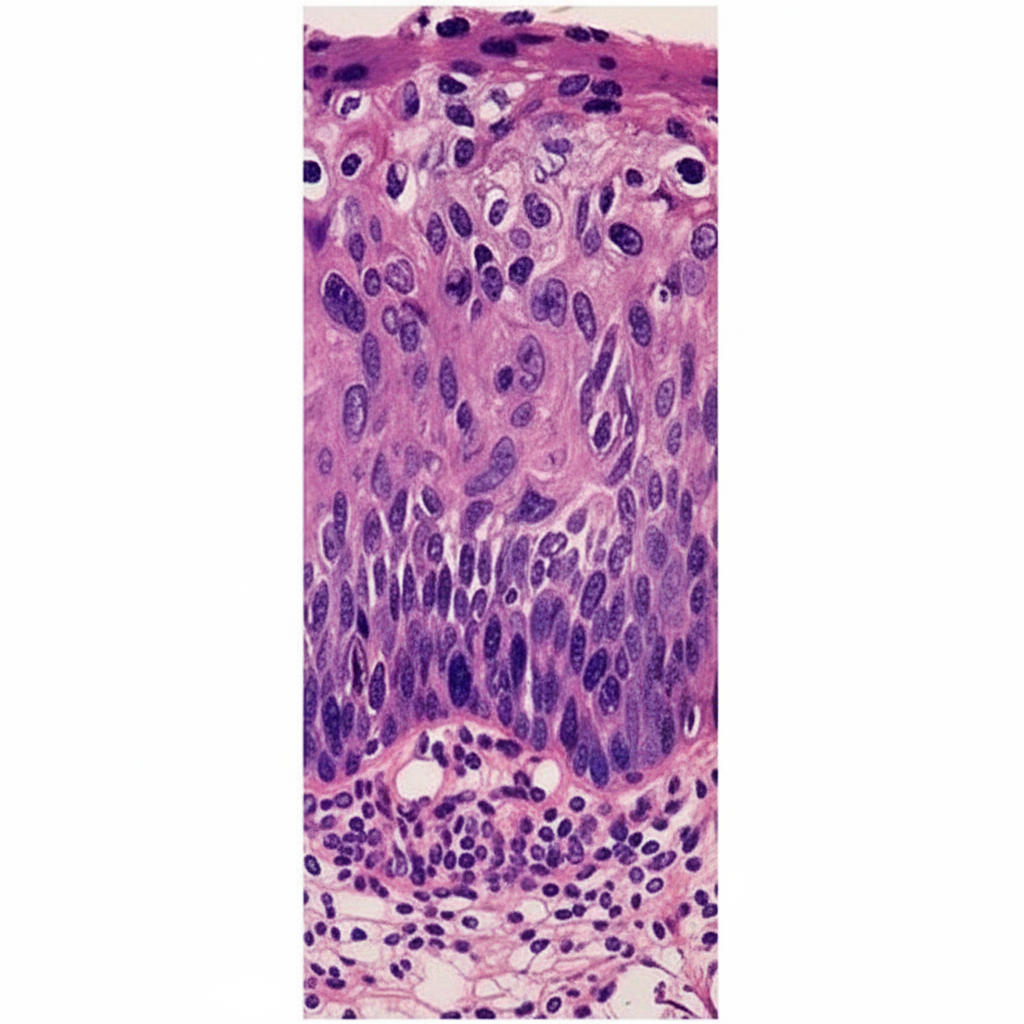
Condyloma acuminata is reported on Pap smear as:
A 50-year-old female presented with a lump in the right breast and was diagnosed with Luminal A carcinoma. Which of the following statements about this cancer is FALSE?
Gleason's scoring is performed for which of the following malignancies?
Which ovarian tumor is typically bilateral?
What is the most important prognostic factor for breast carcinoma?
Oestrogen causes proliferation of which cells in the vaginal epithelium?
Which of the following is NOT true about spermatocytic seminoma?
What is the interpretation of the given cervix biopsy of a 50-year-old lady?
Which testicular tumor is associated with high HCG levels?
Practice by Chapter
Diseases of Male Genital Tract
Practice Questions
Testicular Tumors
Practice Questions
Prostate Pathology
Practice Questions
Diseases of Female Genital Tract
Practice Questions
Cervical Pathology and Neoplasia
Practice Questions
Endometrial Pathology
Practice Questions
Ovarian Diseases and Tumors
Practice Questions
Gestational Trophoblastic Disease
Practice Questions
Placental Pathology
Practice Questions
Sexually Transmitted Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app