
Kidney in Systemic Diseases — MCQs

Which type of amyloid is associated with long-term hemodialysis?
Kimmelstiel-Wilson lesion is characteristic of which condition?
Loss of foot processes seen on electron microscopy of renal biopsy is a classical feature in which of the following?
Class IV lupus nephritis is:
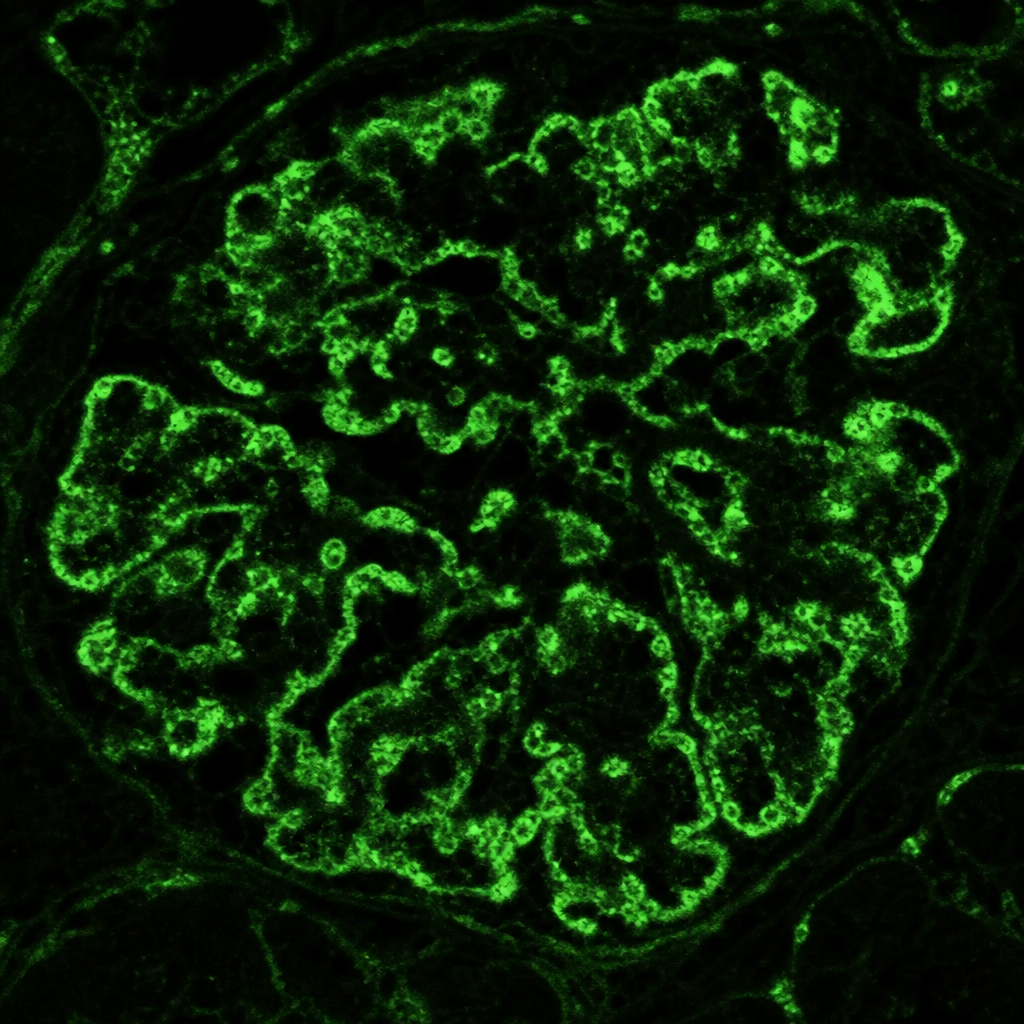
Immunofluorescence staining pattern from a kidney biopsy from a 35-year-old patient presenting with proteinuria has been shown below. What is the most probable cause?
A patient presents with pulmonary hemorrhage and is P-ANCA positive. What is the most likely diagnosis?
All the following are features of Polycystic disease of kidneys EXCEPT:
In a case of glomerulonephritis (GN), C3 is normal in all the following except?
IgA nephropathy is not associated with which of the following?
A 7 year old boy presented with generalized edema. Urine examination revealed marked albuminuria. Serum biochemical examinations showed hypoalbuminemia with hyperlipidemia. Kidney biopsy was undertaken. On light microscopic examination, the kidney appeared normal. Electron microscopic examination is most likely to reveal
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app