
Glomerular Diseases — MCQs

A characteristic feature of nephritic syndrome in children is:
Which of the following is the LEAST common characteristic of nephrotic syndrome?
A kidney biopsy under electron microscopy shows subepithelial 'spike' formation. Which immunofluorescence pattern would confirm membranous nephropathy?
Child with proteinuria, generalized edema, hypoproteinemia, and hyperlipidemia - most common cause is?
Which of the following is NOT a feature of nephrotic syndrome?
In the glomerulus, subendothelial deposits are seen in?
Which of these conditions is classified as a nephritic syndrome?
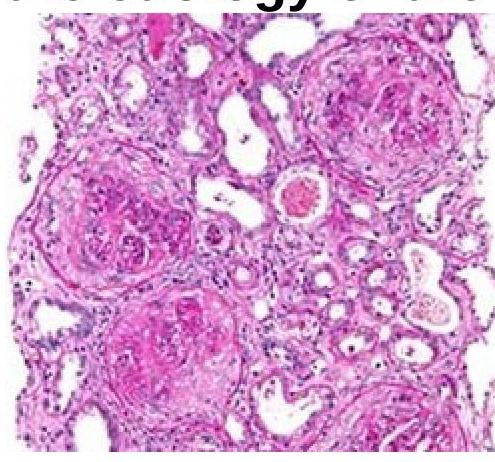
A 51-year-old person came with a complaint of hematuria. On examination, he was normotensive and had pedal edema. Investigations revealed the patient had no glucosuria and had a creatinine value of 9mg%. Renal biopsy is as shown below. Which of the following investigations should be done to identify the etiology of the disease?
Loss of foot processes seen on electron microscopy of renal biopsy is a classical feature in which of the following?
A 7-year-old boy presented with generalized edema. Urine examination revealed marked albuminuria. Serum biochemical examinations showed hypoalbuminemia with hyperlipidemia. Kidney biopsy was undertaken. On light microscopic examination, the kidney appeared normal. Electron microscopic examination is most likely to reveal:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app