
Congenital and Developmental Disorders — MCQs

Which of the following most likely causes a communicating (nonobstructive) hydrocephalus?
Arnold Chiari malformation is characterized by all of the following except:
When should folic acid supplementation start in order to be effective in preventing neural tube defects?
Which of the following is the MOST accurate test for detecting neural tube defects?
A 10 year old child presented with headache, vomiting, gait instability and diplopia. On examination he had papilledema and gait ataxia. The most probable diagnosis is –
Meningomyelocele with progressive hydrocephalus is commonly seen in
Porencephaly refers to -
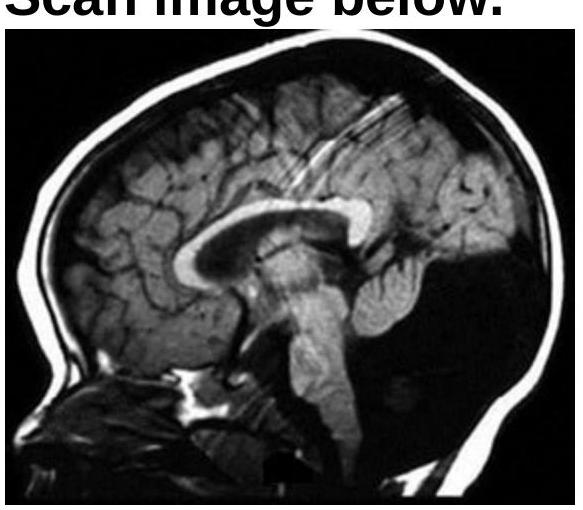
Identify the condition shown in the CT scan image.
A newborn baby presented with a failure to pass meconium in the immediate postnatal period. The pediatrician also notices visible yet ineffective peristalsis, and abdominal distention. A radiological contrast enema demonstrated a narrow conical segment and a dilated proximal bowel. A diagnosis of Hirschsprung disease was made. Which of the following is a cause of the condition in the patient?
A muscle biopsy shows type 1 fiber atrophy and increased internal nuclei on histology. Which additional finding on light microscopy would be most specific for myotonic dystrophy?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app