
Molecular Pathology — MCQs

On this page
On which chromosome is the Her2/neu gene located?
Which of the following is NOT seen in Fragile X syndrome?
Which of the following is true in Klinefelter syndrome?
Which one of the following is not a polygenic disorder?
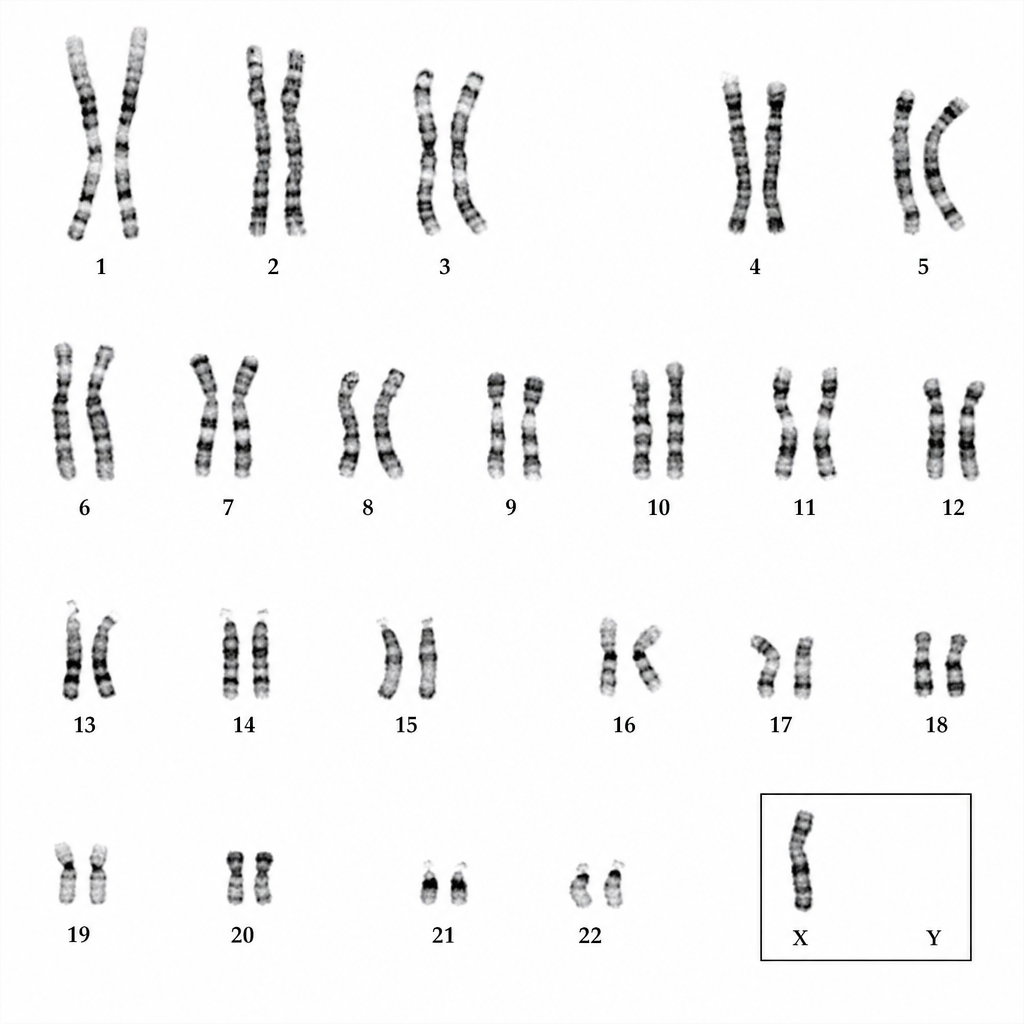
Comment on the diagnosis.
Down's syndrome is most commonly caused by?
What is the most common microdeletion syndrome?
A normal couple has one daughter affected with Cystic fibrosis. They are now planning to have another child. What is the chance of siblings being affected by the disease?
What is the typical number of chromosomes in an individual with Klinefelter syndrome?
Which of the following is false regarding cystic fibrosis?
Practice by Chapter
Principles of Molecular Pathology
Practice Questions
DNA and RNA Analysis Techniques
Practice Questions
Cytogenetics
Practice Questions
Polymerase Chain Reaction Applications
Practice Questions
Next-Generation Sequencing
Practice Questions
Molecular Diagnosis of Infectious Diseases
Practice Questions
Molecular Oncology
Practice Questions
Pharmacogenomics
Practice Questions
Genetic Counseling and Risk Assessment
Practice Questions
Molecular Diagnostics Quality Control
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app