
Molecular Pathology — MCQs

On this page
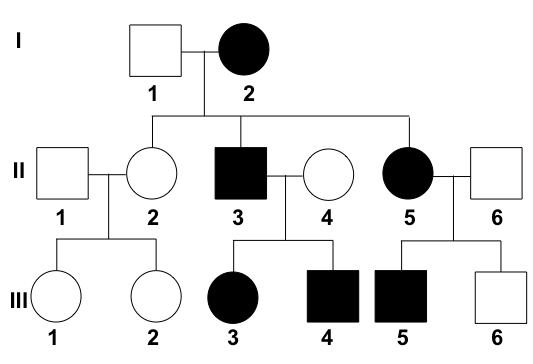
What is the interpretation of the given pedigree chart?
Match the following? a. Trisomy 13 1. Huntington disease b. Trisomy 18 2. Patau syndrome c. Trinucleotide repeat sequence 3. Sickle cell disease d. Hb point mutation of glutamate to valine 4. Edward syndrome
Fluorescence in situ hybridization (FISH) is required in which of the following interpretations of Her2/neu?
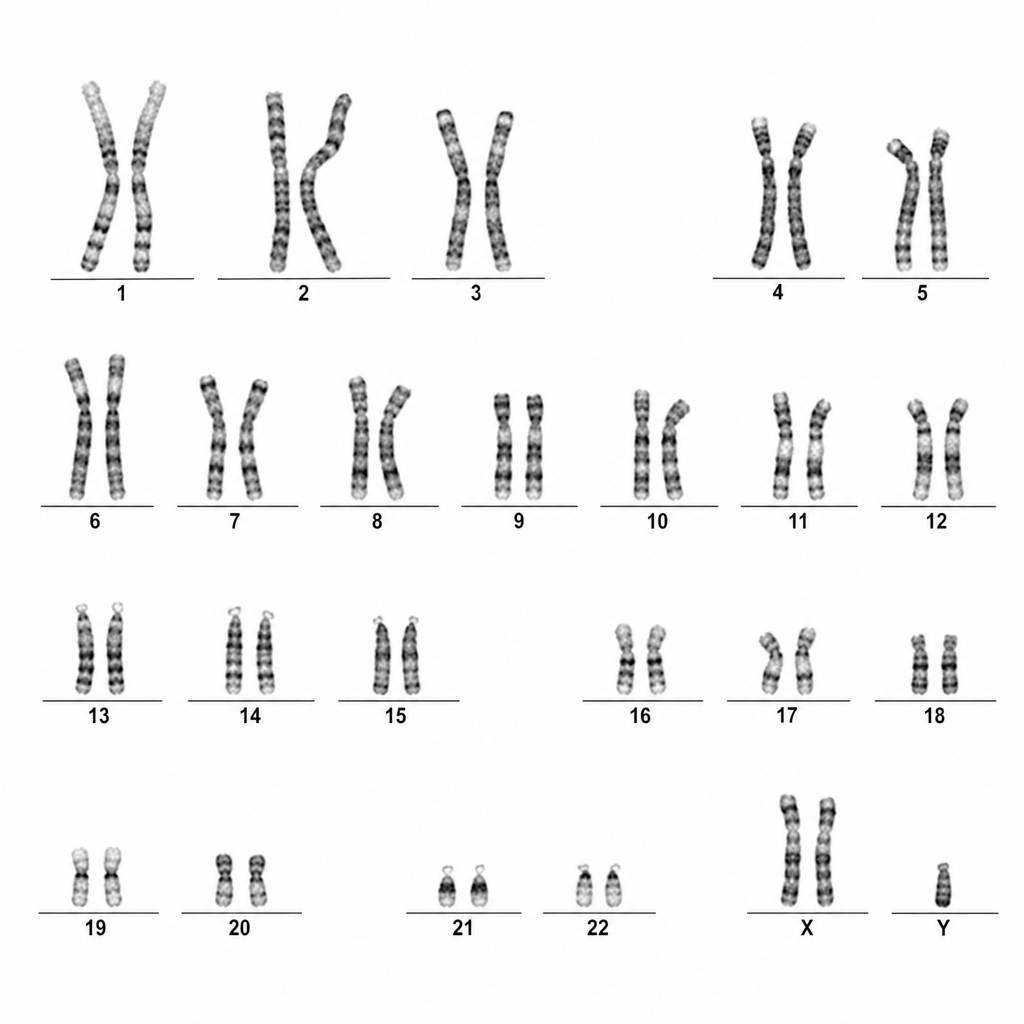
A karyotyping image is given below. What are the clinical features most likely to be expected in such patients?
Which of the following is true? 1. BRCA1 is an oncogene 2. HER2neu is amplified only in a fraction of breast cancer 3. EGFR (+) is seen in non-small cell lung cancer 4. N-MYC is a tumor suppressor gene
Which of the following is an Autosomal Dominant disease?
Barr body is NOT seen in:
Which of the following childhood tumor uses N-myc gene amplification for its prognosis?
A 25-year-old woman with amenorrhea has never had menarche. On physical examination, she is 145 cm (4 ft 9 in) tall. She has a webbed neck, a broad chest, and widely spaced nipples. Strong pulses are palpable in the upper extremities, but there are only weak pulses in the lower extremities. On abdominal MR imaging, her ovaries are small, elongated, and tubular. Which of the following karyotypes is she most likely to have?
BRCA1 gene lies on chromosome
Practice by Chapter
Principles of Molecular Pathology
Practice Questions
DNA and RNA Analysis Techniques
Practice Questions
Cytogenetics
Practice Questions
Polymerase Chain Reaction Applications
Practice Questions
Next-Generation Sequencing
Practice Questions
Molecular Diagnosis of Infectious Diseases
Practice Questions
Molecular Oncology
Practice Questions
Pharmacogenomics
Practice Questions
Genetic Counseling and Risk Assessment
Practice Questions
Molecular Diagnostics Quality Control
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app