
Molecular Pathology — MCQs

On this page
Which of the following statements regarding the inheritance of Neurofibromatosis is FALSE?
Marfan syndrome is due to a mutation of which of the following proteins?
Which of the following types of karyotyping is performed under light microscopy?
Which of the following is NOT a chromosomal breakage syndrome?
Which test is used to differentiate between the chromosomal patterns of a normal cell and a cancer cell?
What is the incidence of Down's syndrome directly proportional to?
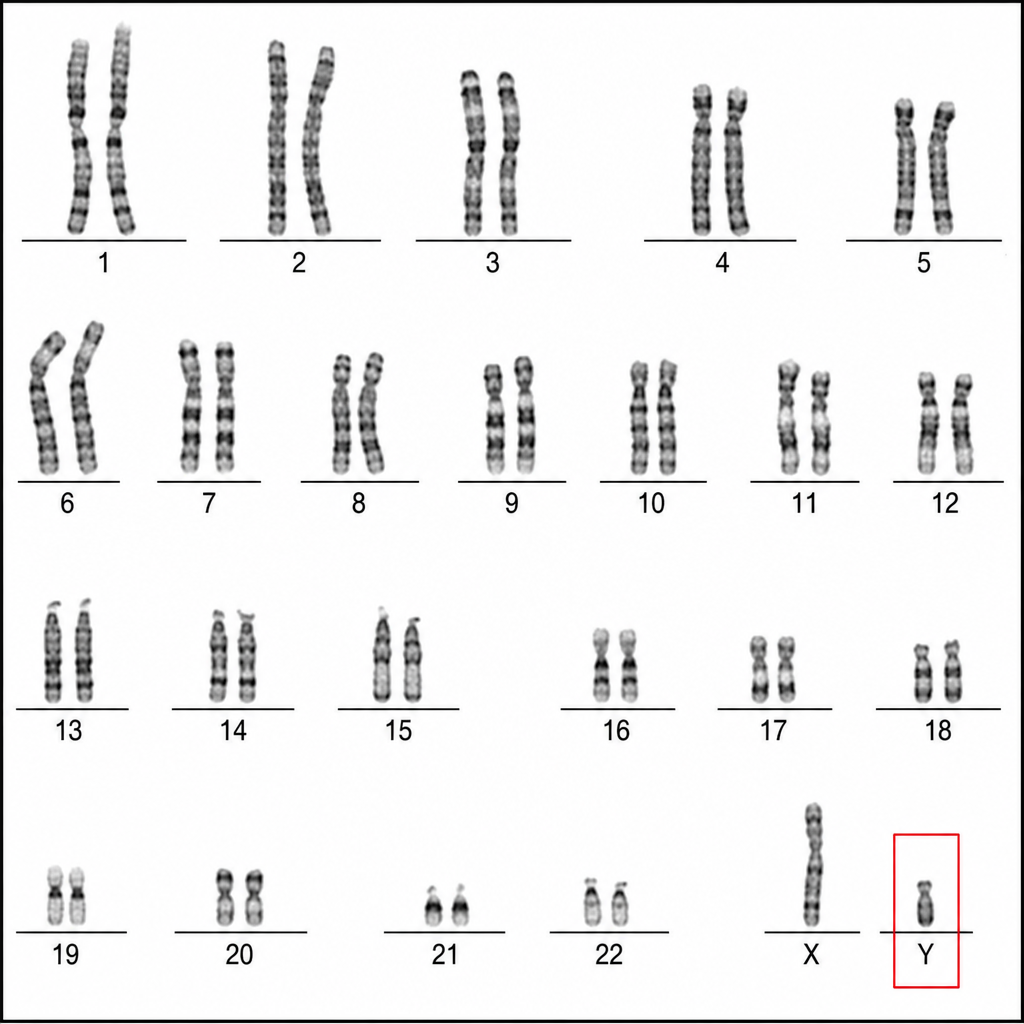
A patient's karyotype shows the following. What is the expected clinical abnormality?
What is the total number of chromosomes typically found in an individual with Turner syndrome?
All of the following are true about tumors associated with BRCA-1 except:
Xeroderma pigmentosum is characterized by
Practice by Chapter
Principles of Molecular Pathology
Practice Questions
DNA and RNA Analysis Techniques
Practice Questions
Cytogenetics
Practice Questions
Polymerase Chain Reaction Applications
Practice Questions
Next-Generation Sequencing
Practice Questions
Molecular Diagnosis of Infectious Diseases
Practice Questions
Molecular Oncology
Practice Questions
Pharmacogenomics
Practice Questions
Genetic Counseling and Risk Assessment
Practice Questions
Molecular Diagnostics Quality Control
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app