
Molecular Pathology — MCQs

On this page
Which of the following is TRUE about Turner's syndrome?
All of the following statements about non-disjunction are true EXCEPT?
What is the term for a single gene defect that causes multiple, seemingly unrelated problems?
Which method is used to detect the BCR-ABL fusion gene?
Which of the following is NOT an advantage of nanotechnology in cancer diagnosis?
A 38-year-old woman shows evidence of early cataracts, hair loss, atrophy of skin, osteoporosis, and accelerated atherosclerosis. This patient has most likely inherited mutations in both alleles of a gene that encodes which of the following types of intracellular proteins?
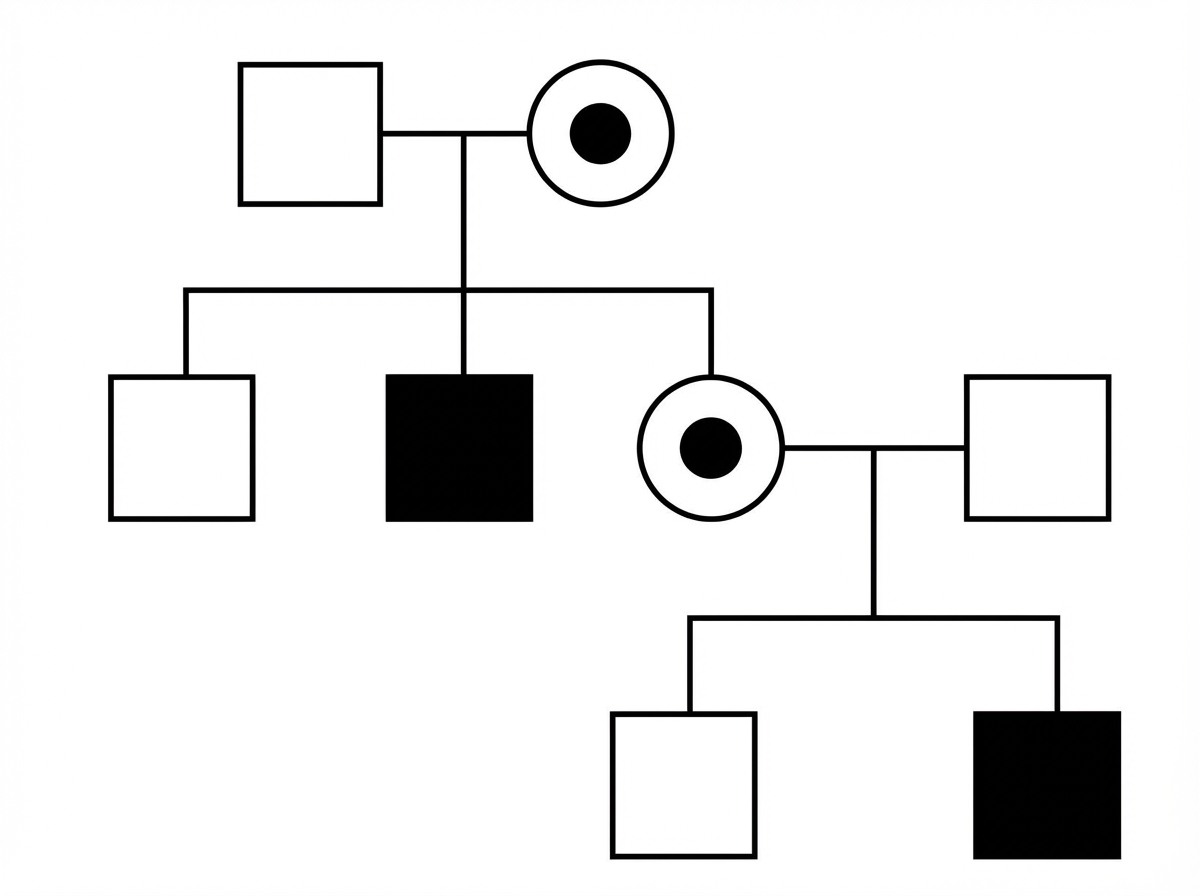
Study the following pedigree. What is the inheritance pattern of the disease in the family?
Turner syndrome is characterized by which chromosomal abnormality?
Translocation between two acrocentric chromosomes occurs with breakpoints near the centromeres, resulting in very large and very small chromosomes. The smaller fragment is typically lost. What is this type of cytogenetic abnormality?
Which of the following chromosomal abnormalities is NOT typically associated with Down Syndrome?
Practice by Chapter
Principles of Molecular Pathology
Practice Questions
DNA and RNA Analysis Techniques
Practice Questions
Cytogenetics
Practice Questions
Polymerase Chain Reaction Applications
Practice Questions
Next-Generation Sequencing
Practice Questions
Molecular Diagnosis of Infectious Diseases
Practice Questions
Molecular Oncology
Practice Questions
Pharmacogenomics
Practice Questions
Genetic Counseling and Risk Assessment
Practice Questions
Molecular Diagnostics Quality Control
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app