
Molecular Pathology — MCQs

On this page
In Down syndrome, the chromosomal abnormality is most commonly due to which of the following?
Most common cause of Down's syndrome is:
45X0 is the chromosomal abnormality seen in which of the following conditions?
Which of the following is an example of a gain-of-function mutation?
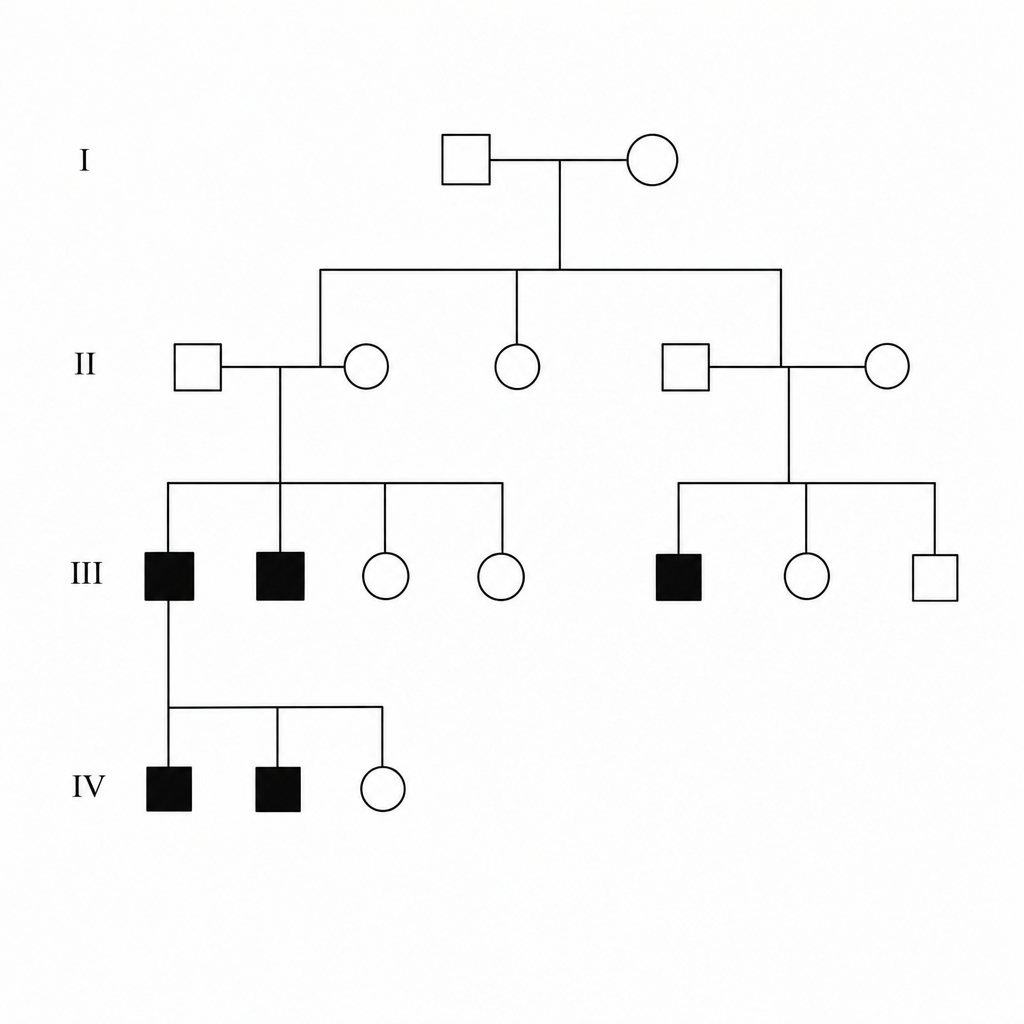
A pedigree chart shows the following pattern of inheritance. The pedigree includes an affected female born to an unaffected father, with unaffected carrier parents producing affected offspring of both sexes. What is the most likely mode of inheritance?
The HER2/neu receptor plays a role in what?
Germline mutations in which of the following genes are not associated with hereditary breast cancer?
Which of the following chromosomes is involved in Patau syndrome?
What is the most common tumor diagnosed in a female patient with tuberous sclerosis?
Beal's syndrome is caused due to a defect in which of the following genes?
Practice by Chapter
Principles of Molecular Pathology
Practice Questions
DNA and RNA Analysis Techniques
Practice Questions
Cytogenetics
Practice Questions
Polymerase Chain Reaction Applications
Practice Questions
Next-Generation Sequencing
Practice Questions
Molecular Diagnosis of Infectious Diseases
Practice Questions
Molecular Oncology
Practice Questions
Pharmacogenomics
Practice Questions
Genetic Counseling and Risk Assessment
Practice Questions
Molecular Diagnostics Quality Control
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app