
Molecular Pathology — MCQs

On this page
In a family, the father has widely spaced eyes, increased facial hair, and deafness. One of the three children has deafness with similar facial features. The mother is normal. Which one of the following patterns of inheritance is least likely in this case?
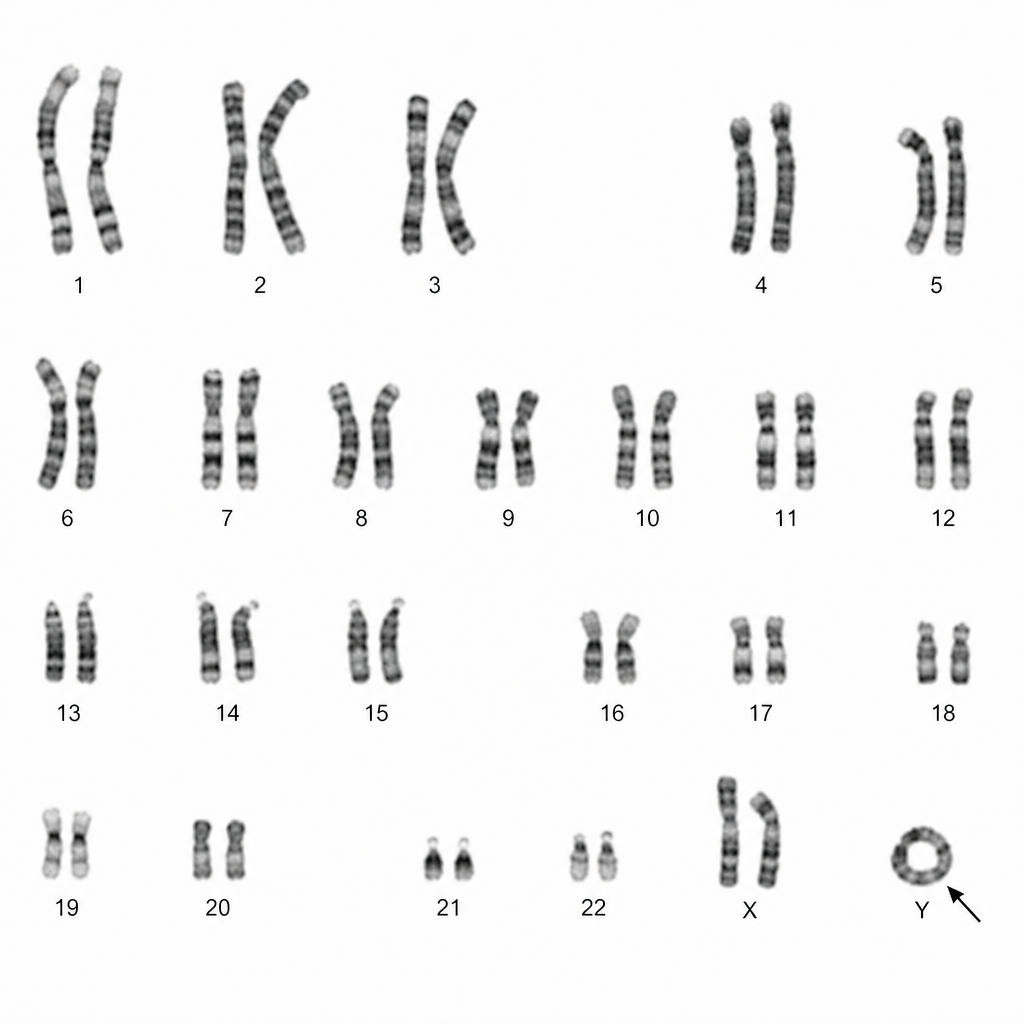
What is the name of this chromosomal abnormality?
A 39-year-old woman is evaluated for severe left hip pain after twisting her leg. She has bony deformities of the lower extremities with limited mobility. The patient had a history of precocious puberty and hyperthyroidism, which was managed by radioiodine therapy. Physical examination shows large, hyperpigmented macules with irregular borders located on the left shoulder, left side of the neck, and left buttock. Which of the following genes is involved in this condition?
Which of the following statements is not true for FISH technique?
Which type of cancer is NOT associated with BRCA2 mutation?
Multifactorial inheritance is seen in which of the following conditions?
Which of the following is false regarding Fragile X syndrome?
Ectrodactyly is an autosomal dominant trait that causes missing middle fingers (lobster claw malformation). A grandfather and grandson both have ectrodactyly, but the intervening father has normal hands by x-ray. Which of the following terms best applies to this family?
Which of the following is the primary cause of phenotypic heterogeneity?
Submicroscopic deletions of any size can be detected by which of the following methods?
Practice by Chapter
Principles of Molecular Pathology
Practice Questions
DNA and RNA Analysis Techniques
Practice Questions
Cytogenetics
Practice Questions
Polymerase Chain Reaction Applications
Practice Questions
Next-Generation Sequencing
Practice Questions
Molecular Diagnosis of Infectious Diseases
Practice Questions
Molecular Oncology
Practice Questions
Pharmacogenomics
Practice Questions
Genetic Counseling and Risk Assessment
Practice Questions
Molecular Diagnostics Quality Control
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app