
Molecular Pathology — MCQs

On this page
Division of a chromosome perpendicular to its normal axis of division leads to which of the following?
Which of the following procedures is routinely used for karyotyping using light microscopy?
Which one of the following is NOT a characteristic feature of an autosomal recessive disorder?
Multifactorial inheritance is most likely to play a role in which of the following conditions?
Von Hippel-Lindau disease is associated with all the following except?
Klinefelter syndrome is associated with all, except:
Which of the following is false regarding Noonan syndrome?
Which syndrome is characterized by the occurrence of both colorectal and endometrial cancers?
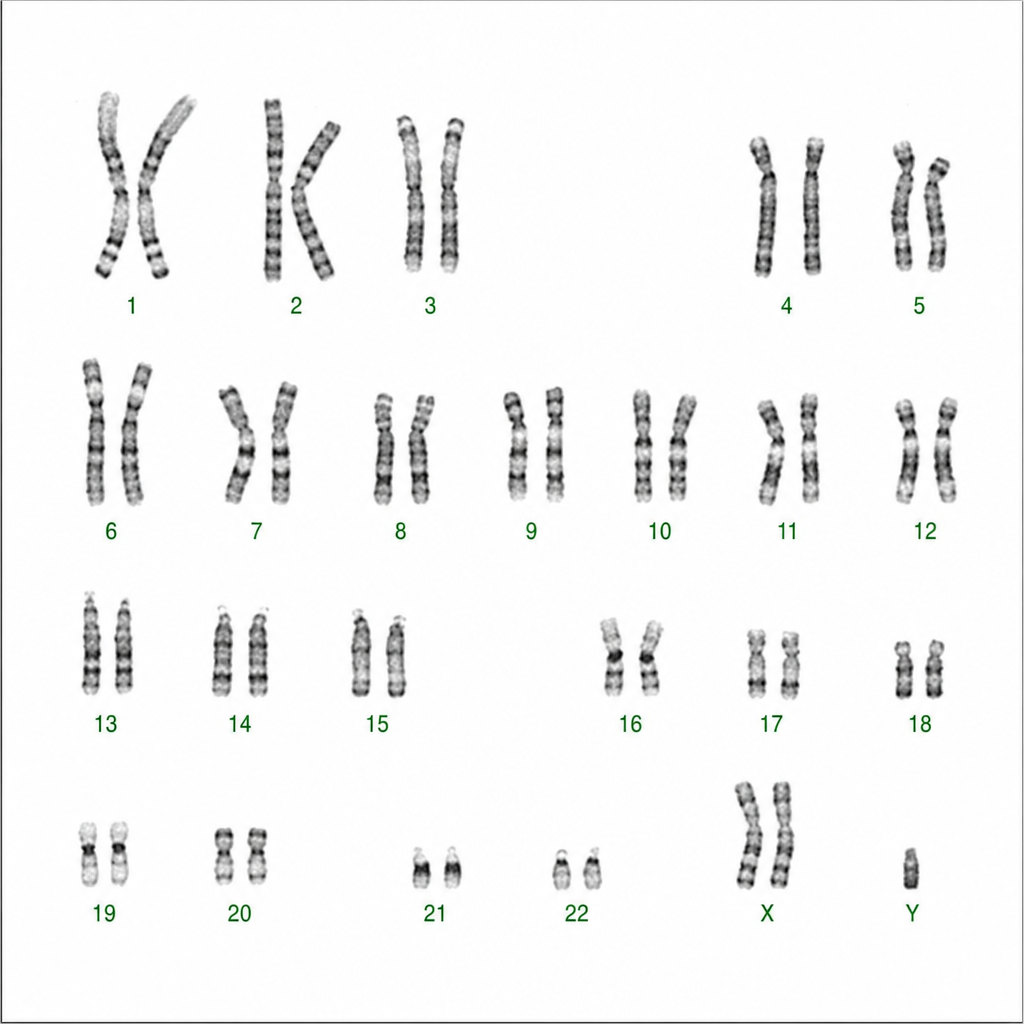
What is the diagnosis suggested by the following karyotype?
Down's syndrome is associated with mental retardation. Which of the following chromosomal abnormalities are not typically found in Down's syndrome?
Practice by Chapter
Principles of Molecular Pathology
Practice Questions
DNA and RNA Analysis Techniques
Practice Questions
Cytogenetics
Practice Questions
Polymerase Chain Reaction Applications
Practice Questions
Next-Generation Sequencing
Practice Questions
Molecular Diagnosis of Infectious Diseases
Practice Questions
Molecular Oncology
Practice Questions
Pharmacogenomics
Practice Questions
Genetic Counseling and Risk Assessment
Practice Questions
Molecular Diagnostics Quality Control
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app