
Molecular Pathology — MCQs

On this page
What is the primary molecular mechanism by which UV light induces carcinogenesis?
A pathologist receives a formalin-fixed paraffin-embedded (FFPE) tissue section. Which technique is most appropriate to identify and localize specific proteins within this section in situ?
Which of the following conditions is not associated with an increased risk of malignancy?
Which of the following is an autosomal dominant metabolic disorder?
A female patient presents with a 2 x 2 cm firm mass in the upper outer quadrant of the breast. She has a family history of ovarian carcinoma. Which investigation needs to be done to assess for a specific gene mutation?
Which of the following conditions is NOT inherited in an autosomal recessive pattern?
Which of the following is true for Klinefelter's syndrome?
Lisch nodules and a pancreatic somatostatinoma are seen in which condition?
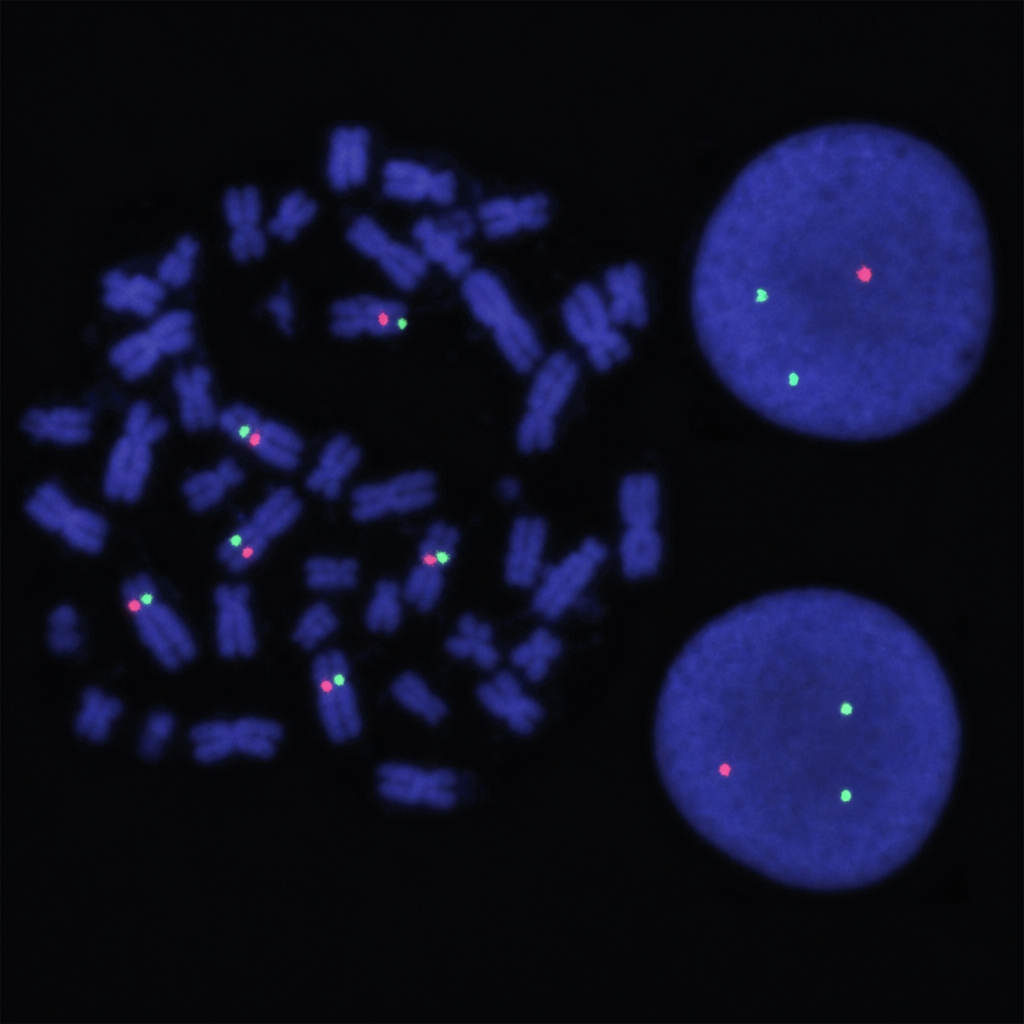
Which genetic abnormality is depicted by the following FISH technique? *Probe legend:* Red probe = BCR (chromosome 22); Green probe = ABL (chromosome 9). Expected normal signal pattern: 2 red + 2 green (separate signals). The image shows an apparent 1-red/2-green interphase pattern, suggesting loss of one red (BCR) probe signal.
Which of the following chromosomal abnormalities is most likely to cause mental retardation?
Practice by Chapter
Principles of Molecular Pathology
Practice Questions
DNA and RNA Analysis Techniques
Practice Questions
Cytogenetics
Practice Questions
Polymerase Chain Reaction Applications
Practice Questions
Next-Generation Sequencing
Practice Questions
Molecular Diagnosis of Infectious Diseases
Practice Questions
Molecular Oncology
Practice Questions
Pharmacogenomics
Practice Questions
Genetic Counseling and Risk Assessment
Practice Questions
Molecular Diagnostics Quality Control
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app