
Liver and Biliary Pathology — MCQs

On this page
All of the following are features of alpha-1 antitrypsin deficiency except?
Which of the following is associated with primary hepatic malignancy?
On stopping alcohol, all the following changes in the liver are reversible EXCEPT?
What is the most common type of gallbladder cancer associated with gallstones?
A 50-year-old male presents with chronic right heart failure and succumbs to his illness. On autopsy, what characteristic changes are seen in the liver?
Centrilobular necrosis in the liver is due to which of the following conditions?
Acetaminophen poisoning causes which of the following changes in the liver?
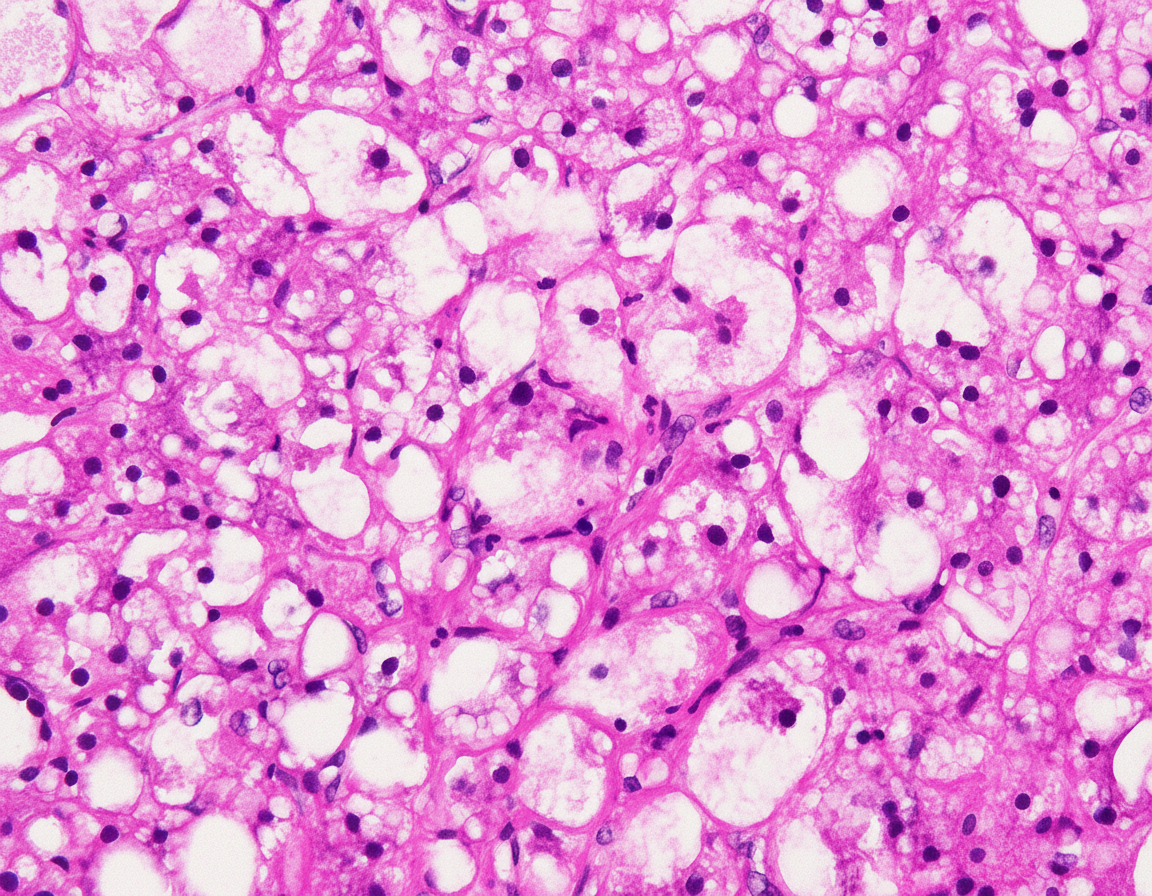
A 45-year-old male with a history of chronic alcoholism presented with pain in the abdomen. Ultrasound suggested fatty liver. A liver biopsy was performed and is shown below. What is your interpretation and likely diagnosis?
An oval lesion is found in the right lobe of the liver in an otherwise asymptomatic 24-year-old female. Surgical resection finds a single well-demarcated lesion that has a prominent, central, stellate white scar. What is the most consistent diagnosis based on this gross appearance?
Which of the following is the inheritance pattern of Caroli's syndrome?
Practice by Chapter
Jaundice and Cholestasis
Practice Questions
Viral Hepatitis
Practice Questions
Alcoholic and Non-alcoholic Fatty Liver Disease
Practice Questions
Drug and Toxin Induced Liver Injury
Practice Questions
Cirrhosis and Its Complications
Practice Questions
Metabolic Liver Diseases
Practice Questions
Liver Tumors
Practice Questions
Gallbladder and Biliary Tract Diseases
Practice Questions
Congenital Liver Diseases
Practice Questions
Liver Transplantation Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app