
Liver and Biliary Pathology — MCQs

On this page
Which of the following statements about fibrolamellar carcinoma is TRUE?
Hemochromatosis affects the following organs EXCEPT?
NCPF is due to:
Mallory's degeneration seen in alcoholic liver disease is a form of which type of degeneration?
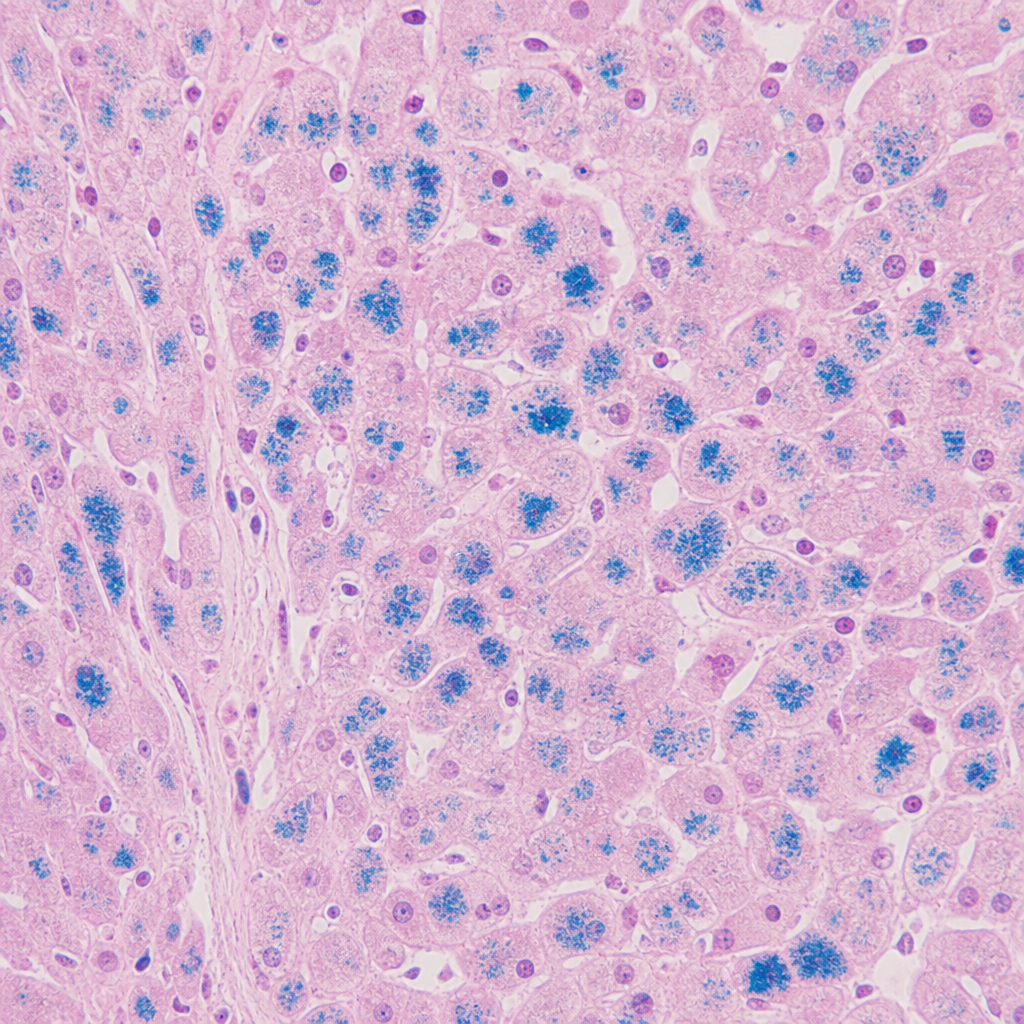
Given below is the histopathology of liver biopsy of hemochromatosis. Which of the following stain is used to detect iron deposition?
Which of the following is NOT a feature of liver damage?
Liver biopsy of an icteric patient shows intensely eosinophilic objects called as Councilman bodies. What is the likely diagnosis of this patient?
Councilman bodies are formed due to which process?
Which of the following conditions is characterized by the presence of large giant cells?
A 25-year-old woman with sickle cell anemia complains of steady pain in her right upper quadrant with radiation to the right shoulder, especially after large or fatty meals. Her physician diagnoses gallstones. Of which of the following compounds are these stones most likely composed?
Practice by Chapter
Jaundice and Cholestasis
Practice Questions
Viral Hepatitis
Practice Questions
Alcoholic and Non-alcoholic Fatty Liver Disease
Practice Questions
Drug and Toxin Induced Liver Injury
Practice Questions
Cirrhosis and Its Complications
Practice Questions
Metabolic Liver Diseases
Practice Questions
Liver Tumors
Practice Questions
Gallbladder and Biliary Tract Diseases
Practice Questions
Congenital Liver Diseases
Practice Questions
Liver Transplantation Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app