
Liver and Biliary Pathology — MCQs

On this page
A 32-year-old male with a history of klebsiella infection presents with right upper quadrant pain and on performing cholecystectomy the following stones were seen. All the following statements are true regarding this condition except: (Recent NEET Pattern 2016-17)
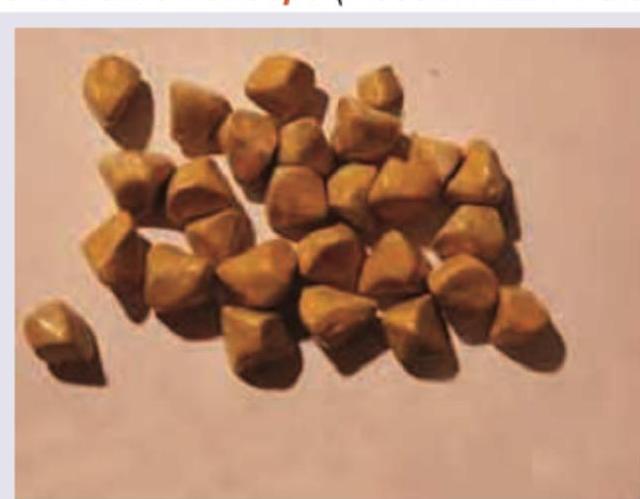
What type of gallstones are shown in the image from a patient with history of acute cholecystitis?
A liver biopsy reveals following findings. What is true about this condition?
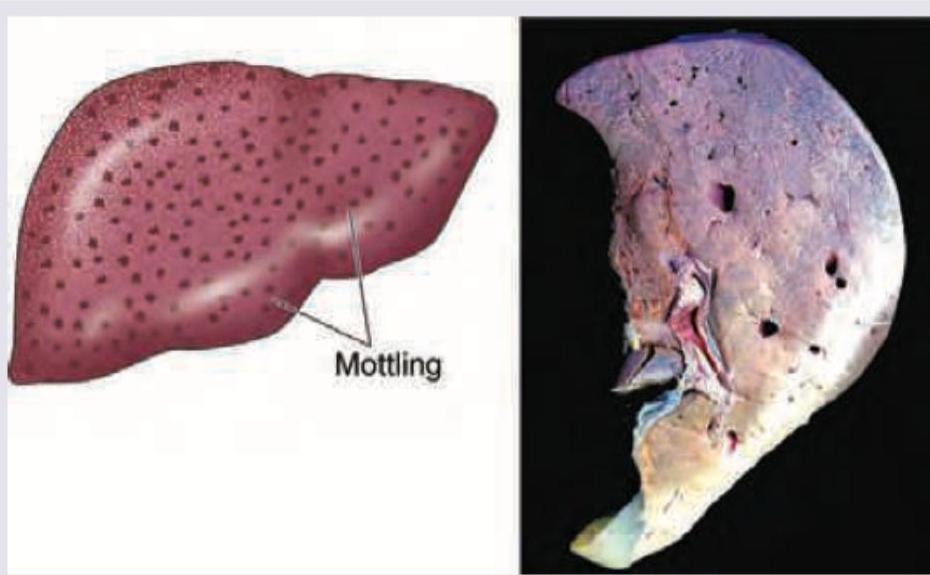
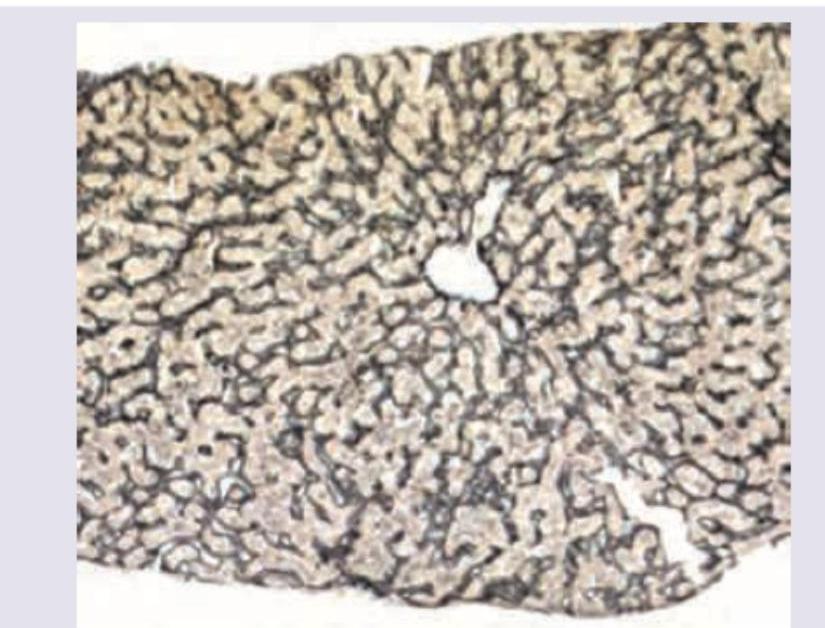
All are true about the sectioned slice of liver except:
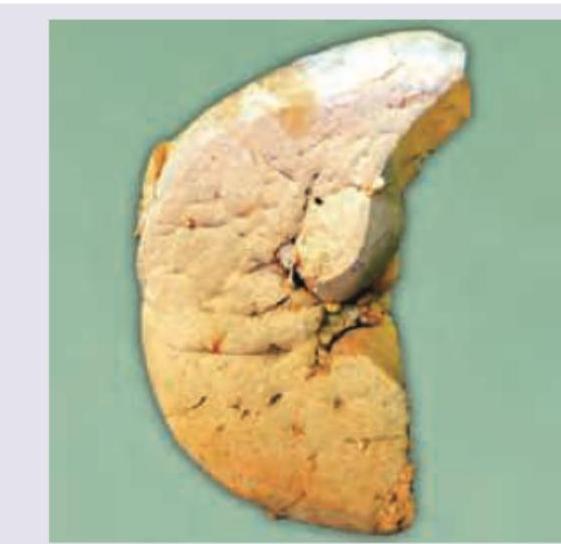
Identify the stain shown in the liver section.
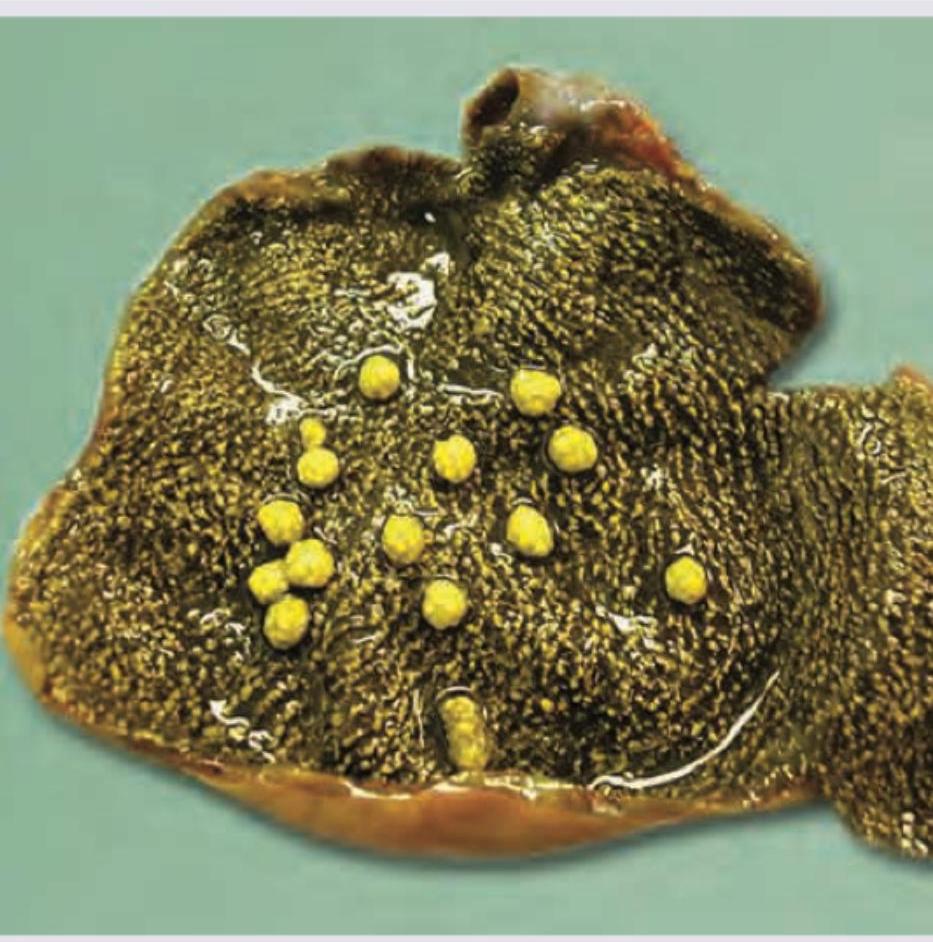
Consider the following: 1. Cholesterolosis 2. Adenomyomatosis 3. Polyposis 4. Cholelithiasis To which of the above does cholecystoses refer to?
Which of the following is NOT correct for ‘strawberry gall bladder’?
Which of the following statements regarding hepatic adenomas are correct? 1. They are almost exclusively seen in females aged 25-50 years 2. They are associated with the use of oral contraceptive pills 3. They do not have any malignant potential 4. Majority are detected incidentally on imaging
A chronic alcoholic patient presents with increasing abdominal girth. A liver biopsy reveals reddish inclusions within the hepatocytes. What are these inclusions composed of?
A 65-year-old man comes to the clinic complaining of abdominal pain for the past 2 months. He describes the pain as a dull, aching, 6/10 pain that is diffuse but worse in the right upper quadrant (RUQ). His past medical history is significant for diabetes controlled with metformin and a cholecystectomy 10 years ago. He reports fatigue and a 10-lb weight loss over the past month that he attributes to poor appetite; he denies fever, nausea/vomiting, palpitations, chest pain, or bowel changes. Physical examination is significant for mild scleral icterus and tenderness at the RUQ. Further workup reveals a high-grade malignant vascular neoplasm of the liver. What relevant detail would you expect to find in this patient’s history?
Practice by Chapter
Jaundice and Cholestasis
Practice Questions
Viral Hepatitis
Practice Questions
Alcoholic and Non-alcoholic Fatty Liver Disease
Practice Questions
Drug and Toxin Induced Liver Injury
Practice Questions
Cirrhosis and Its Complications
Practice Questions
Metabolic Liver Diseases
Practice Questions
Liver Tumors
Practice Questions
Gallbladder and Biliary Tract Diseases
Practice Questions
Congenital Liver Diseases
Practice Questions
Liver Transplantation Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app