
Liver and Biliary Pathology — MCQs

On this page
Which of the following statements are true about alpha-1-antitrypsin deficiency?
In post-hepatic jaundice, the concentration of conjugated bilirubin in the blood is higher than that of unconjugated bilirubin because:
In chronic viral hepatitis, what does grading refer to?
All are important mechanisms in the formation of lithogenic bile EXCEPT?
Increased IgA levels are seen in which of the following conditions?
Vinyl chloride exposure is associated with which of the following malignancies?
A newborn presents with jaundice, conjugated hyperbilirubinemia, intrahepatic cholestasis, and elevated alkaline phosphatase. Liver biopsy reveals eosinophilic, PAS-positive cytoplasmic granules in hepatocytes. What is the most likely diagnosis?
A 58-year-old male with history of multiple sexual partners presented with anorexia and jaundice. The biopsy shows ground-glass opacity in the cells. What is the most probable diagnosis?
A liver biopsy shows ballooning degeneration of hepatocytes, Mallory-Denk bodies, and neutrophilic infiltration. The patient has a history of chronic alcohol abuse. What is the most likely diagnosis?
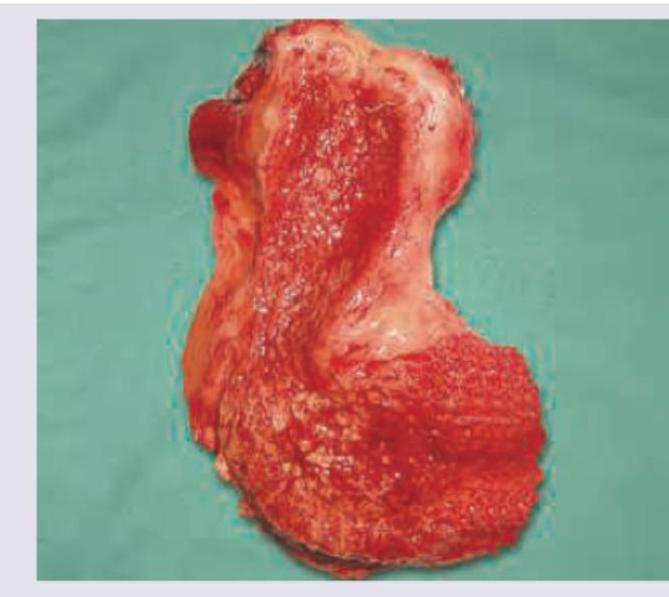
Comment on the diagnosis of the gallbladder specimen provided: (Recent NEET Pattern 2016-17)
Practice by Chapter
Jaundice and Cholestasis
Practice Questions
Viral Hepatitis
Practice Questions
Alcoholic and Non-alcoholic Fatty Liver Disease
Practice Questions
Drug and Toxin Induced Liver Injury
Practice Questions
Cirrhosis and Its Complications
Practice Questions
Metabolic Liver Diseases
Practice Questions
Liver Tumors
Practice Questions
Gallbladder and Biliary Tract Diseases
Practice Questions
Congenital Liver Diseases
Practice Questions
Liver Transplantation Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app