
Liver and Biliary Pathology — MCQs

On this page
What is the most common inherited disorder of cholangiocyte injury?
Which of the following conditions typically shows a normal liver biopsy?
Which of the following is not a histomorphological feature of cirrhosis of the liver?
Which of the following is NOT a histopathological feature of extrahepatic biliary atresia?
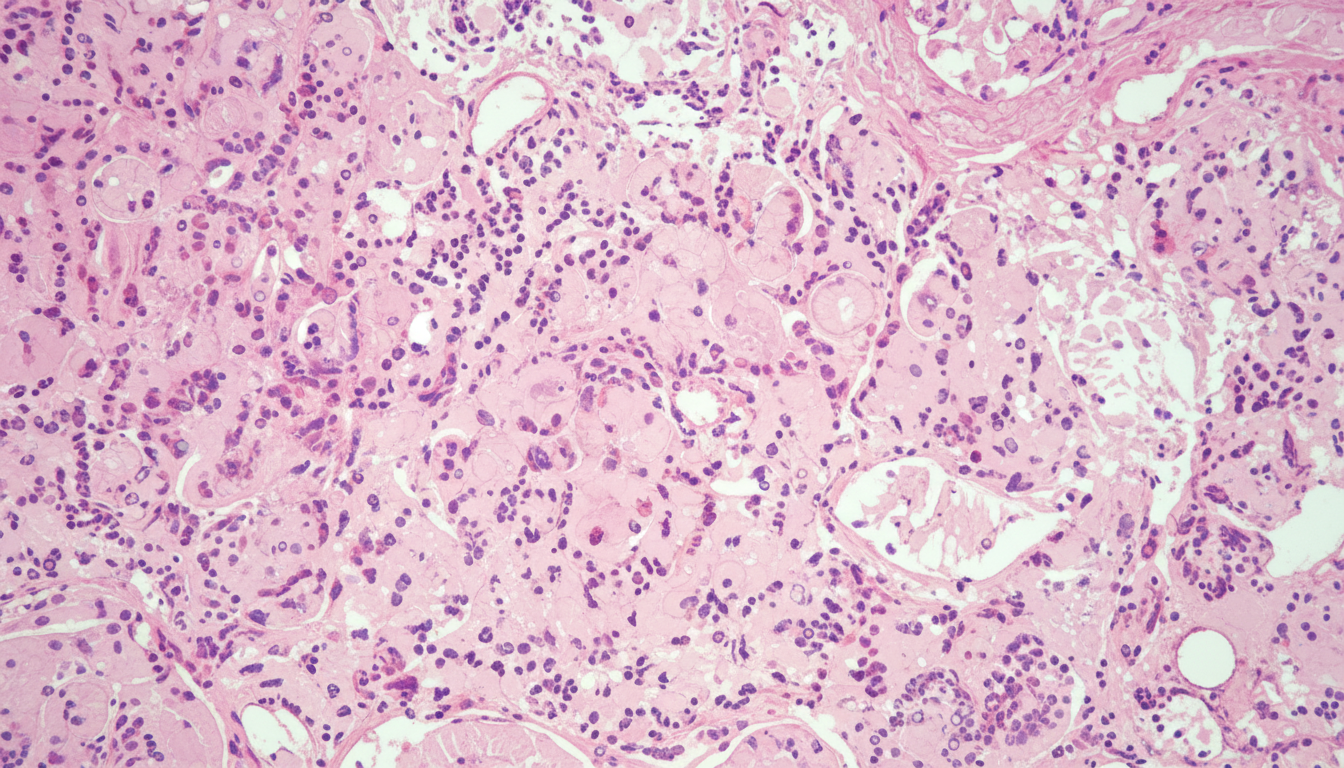
A 43-year-old man has experienced progressive fatigue, pruritus, and icterus for 4 months. A colectomy was performed 5 years ago for the treatment of ulcerative colitis. On physical examination, he has generalized jaundice. The abdomen is not distended; on palpation, there is no abdominal pain and there are no masses. Laboratory studies show a serum alkaline phosphatase level of 285 U/L and an elevated titer of anti-neutrophil cytoplasmic antibodies. Cholangiography shows widespread intrahepatic biliary tree obliteration and a beaded appearance in the remaining ducts. Which of the following morphologic features is most likely to be present in his liver?
A patient presents with icterus and absent urine urobilinogen. What does this indicate?
Unconjugated hyperbilirubinemia is seen in all of the following except:
A 44-year-old patient presented with jaundice and had a needle prick injury 2 years back. Based on the provided histological features of a liver biopsy, classify the type of hepatitis.
Ballooning of hepatocytes is not associated with which of the following conditions?
Which clinical test is done to assess hepatic function related to bleeding disorders?
Practice by Chapter
Jaundice and Cholestasis
Practice Questions
Viral Hepatitis
Practice Questions
Alcoholic and Non-alcoholic Fatty Liver Disease
Practice Questions
Drug and Toxin Induced Liver Injury
Practice Questions
Cirrhosis and Its Complications
Practice Questions
Metabolic Liver Diseases
Practice Questions
Liver Tumors
Practice Questions
Gallbladder and Biliary Tract Diseases
Practice Questions
Congenital Liver Diseases
Practice Questions
Liver Transplantation Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app