
Liver and Biliary Pathology — MCQs

On this page
Anti-LKM-2 autoantibody is seen in drug-induced liver injury. It is directed against which of the following structures?
Amyloid deposits in the liver are initially seen in which location?
What is the commonest benign tumor of the liver?
All of the following are true about fibrolamellar hepatocellular carcinoma except:
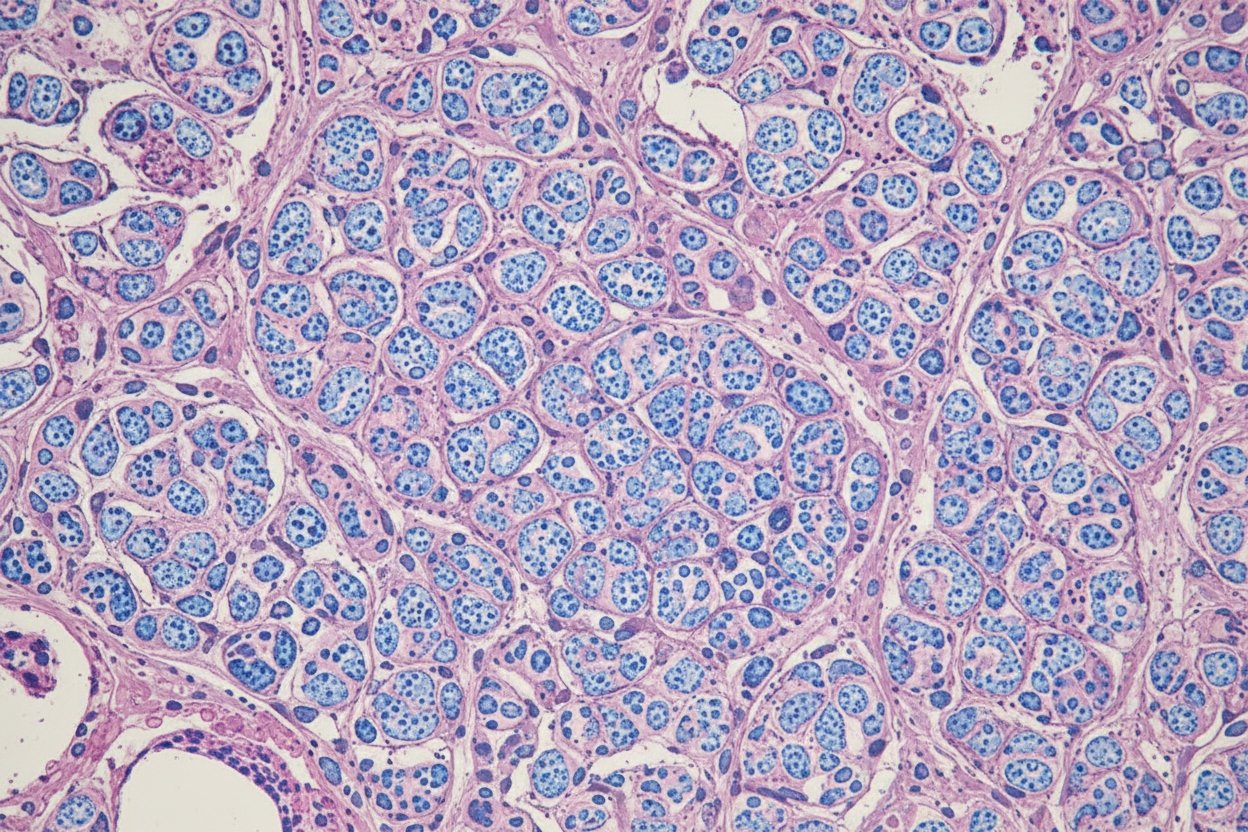
Given below is the histopathology of a liver biopsy of a patient with hemochromatosis. Which of the following special stains has been used?
Which of the following conditions is characterized by unconjugated hyperbilirubinemia with increased urobilinogen?
Fatty liver is due to accumulation of which substance?
Which of the following conditions may not cause microvesicular steatosis?
"Crumbled egg appearance" in liver is seen in which of the following conditions?
What is the most important risk factor for hepatocellular carcinoma?
Practice by Chapter
Jaundice and Cholestasis
Practice Questions
Viral Hepatitis
Practice Questions
Alcoholic and Non-alcoholic Fatty Liver Disease
Practice Questions
Drug and Toxin Induced Liver Injury
Practice Questions
Cirrhosis and Its Complications
Practice Questions
Metabolic Liver Diseases
Practice Questions
Liver Tumors
Practice Questions
Gallbladder and Biliary Tract Diseases
Practice Questions
Congenital Liver Diseases
Practice Questions
Liver Transplantation Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app