
Liver and Biliary Pathology — MCQs

On this page
A 40-year-old obese female presents with fullness of the right upper quadrant of the abdomen. Her medical history is significant for Type 2 diabetes mellitus and hyperlipidemia. A liver biopsy is most likely suggestive of which of the following diagnoses?
Which of the following is not a feature of Alcoholic liver disease?
Which of the following is NOT an alteration in liver function tests seen in bacterial sepsis?
Which of the following features in a liver biopsy is characteristic of alpha-1 antitrypsin deficiency?
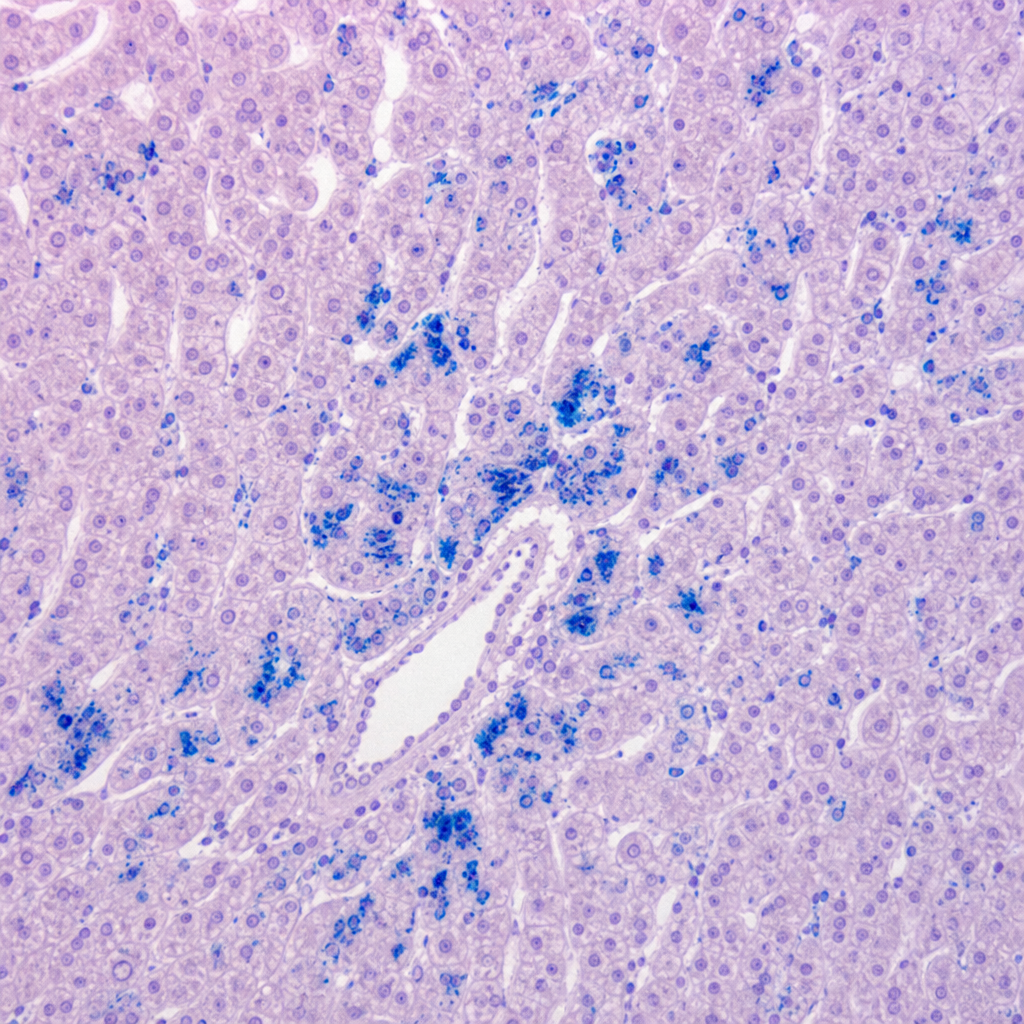
A 40-year-old male presented with cirrhosis. What special stain is used in the histology slide shown below?
A 40-year-old man presents with yellow skin and sclerae, abdominal tenderness, and dark urine. Physical examination reveals jaundice and mild hepatomegaly. Laboratory studies show elevated serum bilirubin (3.1 mg/dL), decreased serum albumin (2.5 g/dL), and prolonged prothrombin time (17 seconds). Serologic tests reveal antibodies to hepatitis B core antigen (IgG anti-HBcAg). The serum is also positive for HBsAg and HBeAg. What glycoprotein on virally infected hepatocytes provides a target for cell-mediated cytotoxicity in this patient?
A 61-year-old man with a history of chronic viral hepatitis has noted a 6-kg weight loss over the past 5 months. Physical examination shows no masses or palpable lymphadenopathy. An abdominal CT scan shows a nodular liver with a 10-cm mass in the right lobe. A stool guaiac test result is negative. An elevation in which of the following laboratory tests is most likely to be present in this man?
A patient with right heart failure secondary to tricuspid regurgitation is found to have increased liver enzymes. USG shows enlargement of the liver. If the patient is developing 'nutmeg liver', what is the most likely etiology?
Cirrhosis of the liver with portal hypertension occurs in all of the following conditions except:
Which of the following viruses does not cause chronic hepatitis?
Practice by Chapter
Jaundice and Cholestasis
Practice Questions
Viral Hepatitis
Practice Questions
Alcoholic and Non-alcoholic Fatty Liver Disease
Practice Questions
Drug and Toxin Induced Liver Injury
Practice Questions
Cirrhosis and Its Complications
Practice Questions
Metabolic Liver Diseases
Practice Questions
Liver Tumors
Practice Questions
Gallbladder and Biliary Tract Diseases
Practice Questions
Congenital Liver Diseases
Practice Questions
Liver Transplantation Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app