
Liver and Biliary Pathology — MCQs

On this page
A child presents with hepatosplenomegaly. Histological examination shows foam cells due to lipid accumulation. What is the most likely diagnosis?
On histopathological examination of liver from a chronic alcoholic, the following image is observed. Which special stain is the best choice to confirm the diagnosis?
A 52-year-old male with a 20-year history of alcohol use disorder presents with abdominal distension, jaundice, and spider angiomata. Liver function tests show elevated bilirubin and low albumin. A liver biopsy is performed and the special stain result is shown in Image 2. The bridging pattern of fibrosis seen in this image most directly results from activation of which cell type?
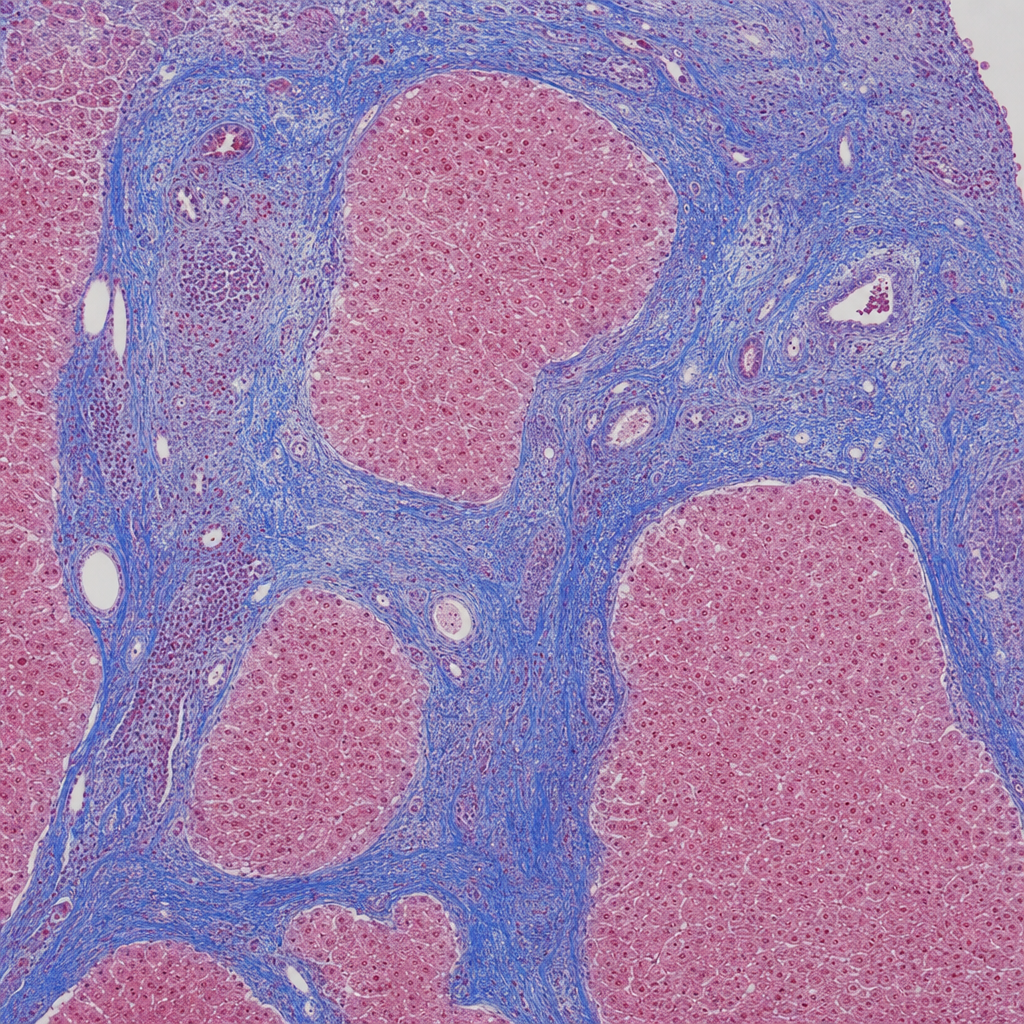
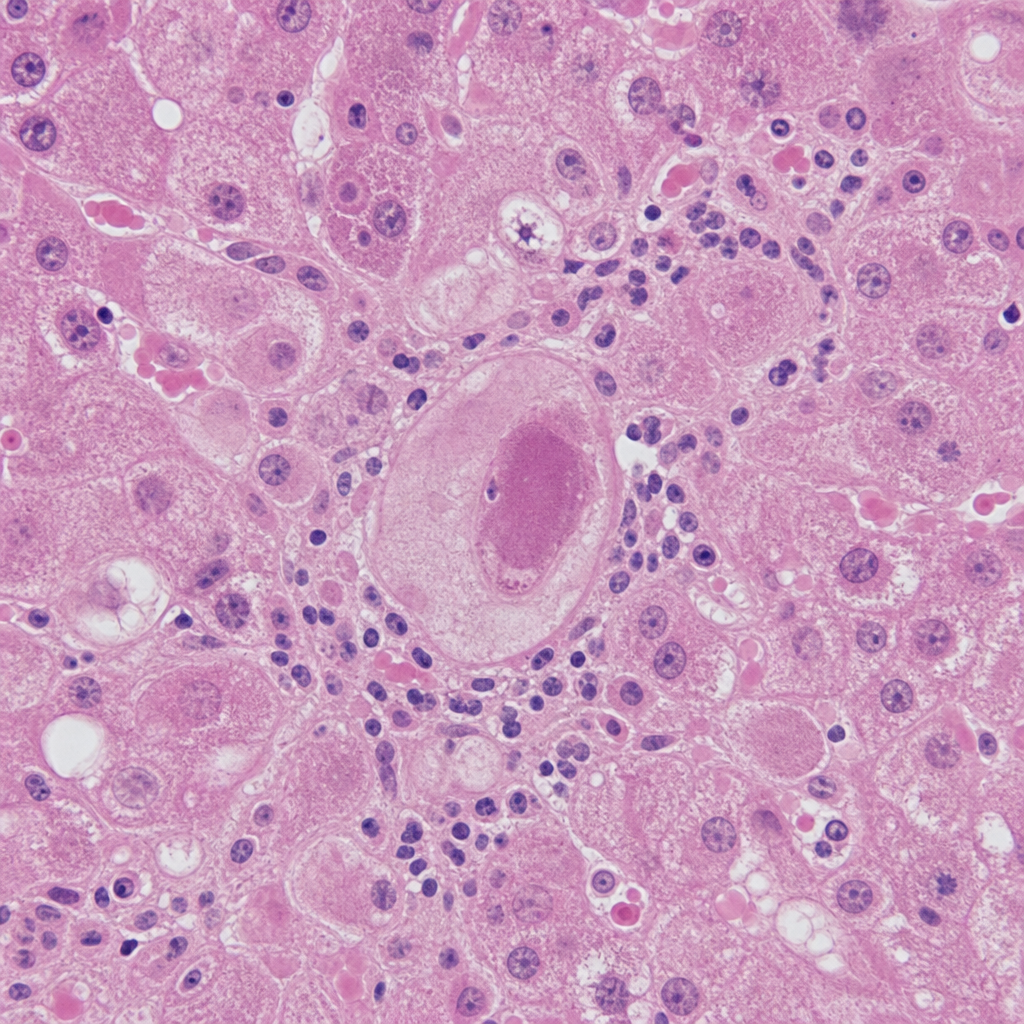
A 55-year-old male with a 20-year history of heavy alcohol consumption presents with jaundice, ascites, and haematemesis. Liver function tests show markedly elevated bilirubin and low albumin. He has spider naevi and palmar erythema on examination. A gross pathology specimen of the liver is shown (Image 2). Which of the following histological features, if present on biopsy of this liver, would most strongly indicate an active ongoing injurious process rather than end-stage fibrosis alone?
Overgrowth of the bile duct in a localized region is termed as:
Kernicterus is invariably associated with which of the following conditions?
Which of the following is NOT a tumor marker for hepatocellular carcinoma?
Extrahepatic cholestasis is associated with which of the following findings?
Which of the following is NOT a characteristic of hepatic adenoma?
Which of the following statements is NOT true about hepatoblastoma?
Practice by Chapter
Jaundice and Cholestasis
Practice Questions
Viral Hepatitis
Practice Questions
Alcoholic and Non-alcoholic Fatty Liver Disease
Practice Questions
Drug and Toxin Induced Liver Injury
Practice Questions
Cirrhosis and Its Complications
Practice Questions
Metabolic Liver Diseases
Practice Questions
Liver Tumors
Practice Questions
Gallbladder and Biliary Tract Diseases
Practice Questions
Congenital Liver Diseases
Practice Questions
Liver Transplantation Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app