
Inflammation and Repair — MCQs

On this page
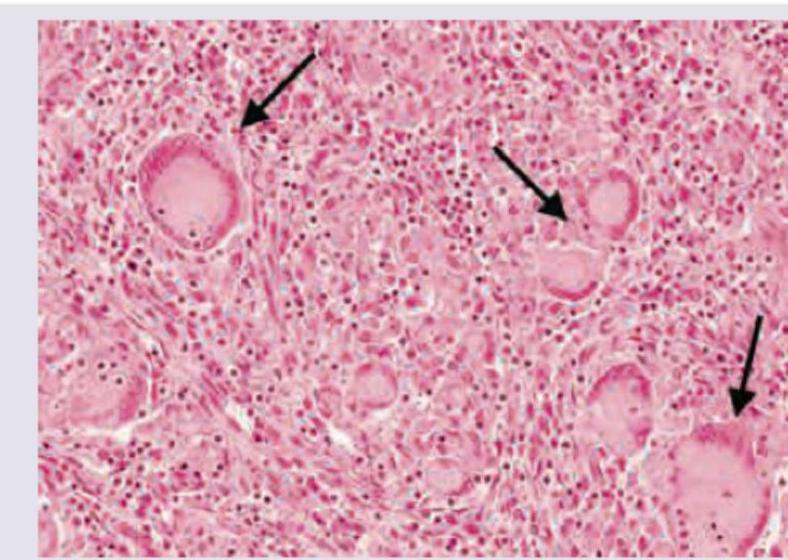
The image shows presence of which cells?
The ratio for Type-I to Type-III collagen during maturation of collagen in remodelling phase is :
The maximum tensile strength that a wound can reach after healing is complete, in comparison to normal skin, is
Langhans' giant cells are characteristically seen in
Hypertrophic scar is characterized by the following, except
Which of the following factors is labelled as cytokine in the pathogenesis of Systemic Inflammatory Response Syndrome (SIRS)?
A 20 year old female was operated for perforation peritonitis and after closing the rectus sheath her abdominal wound was left open to heal with proliferative granulation tissue which contracted and epithelialized to form a scar. This patient had undergone healing by:
Which one of the following factors is NOT involved in the pathogenesis of Systemic inflammatory response syndrome (SIRS)?
What is the correct order of the normal phases of wound healing?
Arrange the following cellular events of inflammation in the correct sequence: 1. Rolling 2. Cytokine-mediated integrin activation 3. Adhesion 4. Migration
Practice by Chapter
Acute Inflammation: Vascular Events
Practice Questions
Acute Inflammation: Cellular Events
Practice Questions
Chemical Mediators of Inflammation
Practice Questions
Chronic Inflammation
Practice Questions
Granulomatous Inflammation
Practice Questions
Systemic Effects of Inflammation
Practice Questions
Wound Healing
Practice Questions
Tissue Regeneration
Practice Questions
Fibrosis and Repair
Practice Questions
Resolution of Inflammation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app