
Inflammation and Repair — MCQs

On this page
Arrange the following steps in order of the events occurring first to last: Margination, Rolling, Stasis, Pavementing?
Which of the following eicosanoids cause vasoconstriction and increase vascular permeability?
Which of the following is NOT a pro-inflammatory cytokine?
Multinucleated giant cells are least likely to be found in which of the following disorders?
Rubor (redness) during inflammation is primarily due to:
In the inflammatory process, what effect do prostaglandins E1 and E2 have?
Esterase inhibitor deficiency causes which of the following conditions?
A 29-year-old carpenter receives a traumatic laceration to her left arm. Which of the following is the most important factor that determines whether this wound will heal by primary or secondary intention?
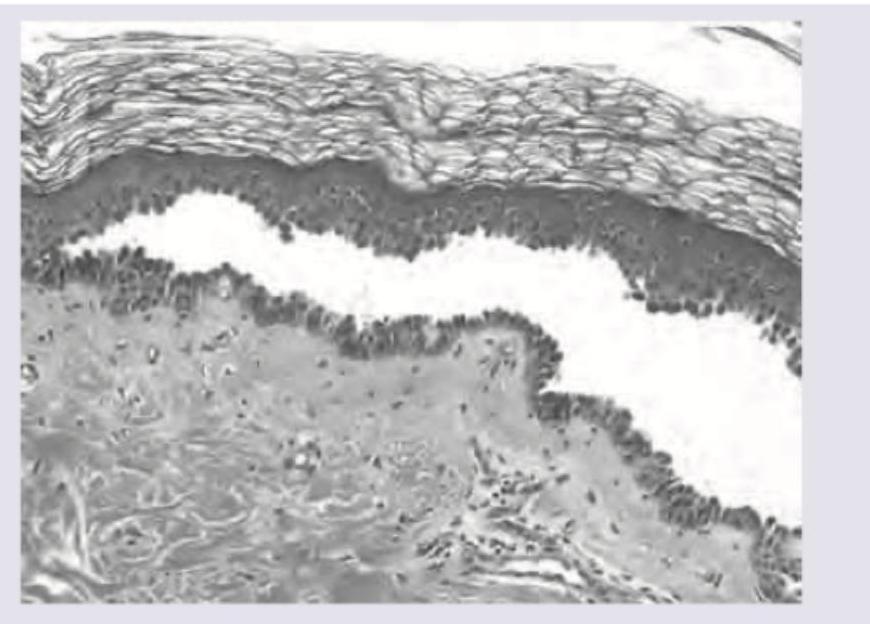
The morphological pattern of inflammation shown here is:
Which of the following statements regarding keloid formation is true?
Practice by Chapter
Acute Inflammation: Vascular Events
Practice Questions
Acute Inflammation: Cellular Events
Practice Questions
Chemical Mediators of Inflammation
Practice Questions
Chronic Inflammation
Practice Questions
Granulomatous Inflammation
Practice Questions
Systemic Effects of Inflammation
Practice Questions
Wound Healing
Practice Questions
Tissue Regeneration
Practice Questions
Fibrosis and Repair
Practice Questions
Resolution of Inflammation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app