
Granulomatous Inflammation — MCQs

A 45-year old patient presented with fever, night sweats and weight loss. On X-ray, a mass was seen in apical lobe. On histopathology, caseous necrosis was present. What is the name of underlying process?
Which of the following is characteristically associated with sarcoidosis?
Granuloma is a pathological feature of all, except which of the following?
Which is NOT a feature of chronic inflammation?
The principal cell in a granuloma is
What is the primary reason for the development of granuloma formation in tertiary syphilis?
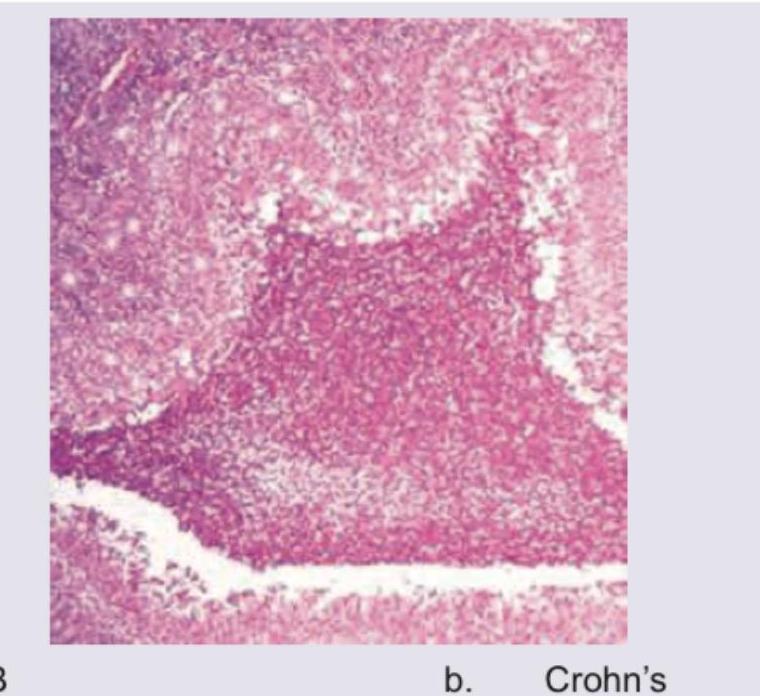
The image shows a histological section of intestinal tissue with a granuloma. What is the most likely diagnosis?
Which of the following does not cause granulomatous inflammation?
Which statement about macrophages is incorrect?
Most important for diapedesis is
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app