
Infectious Diseases — MCQs

On this page
What is the classic histopathological finding in chancroid?
Which feature best differentiates granuloma inguinale from lymphogranuloma venereum?
Which staining technique is considered the most reliable for detecting Cytomegalovirus (CMV) inclusions in tissue samples?
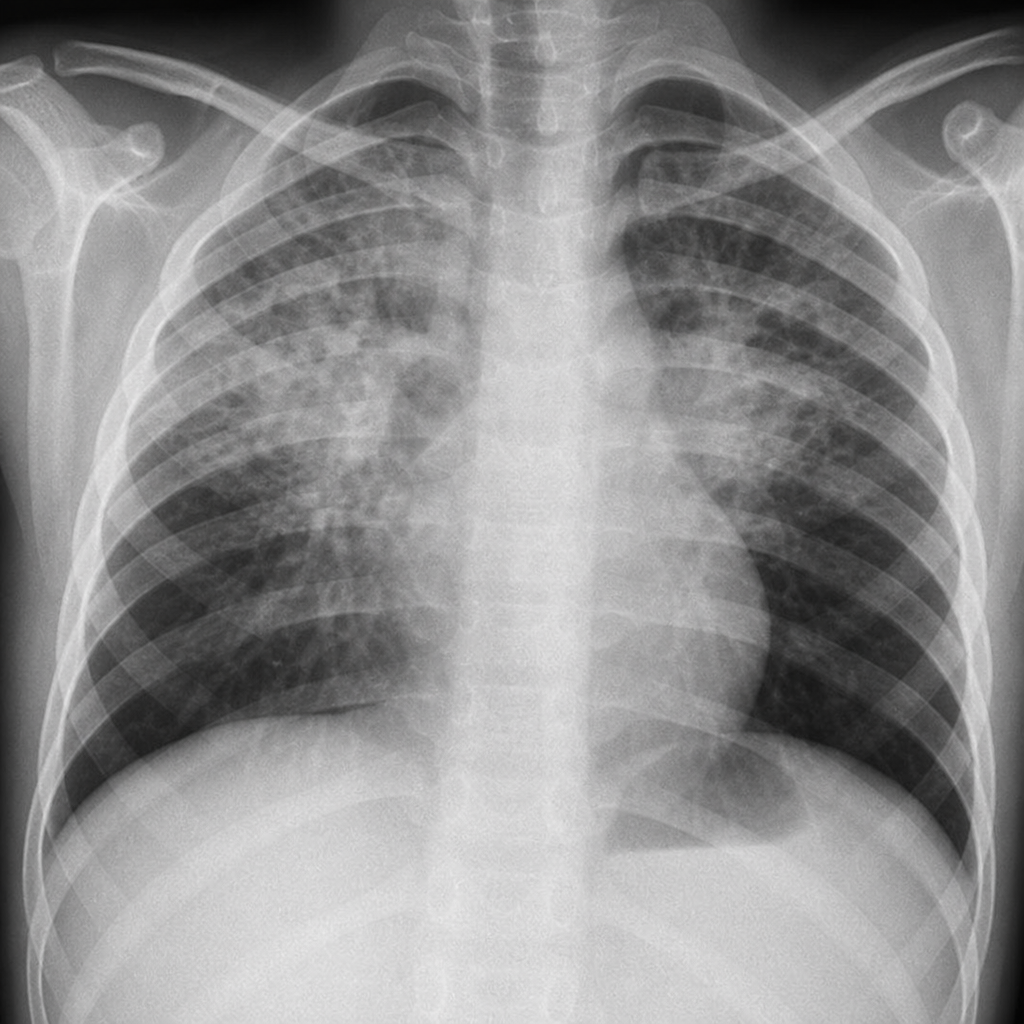
An 11-year-old boy presented with a cough for 15 days and bilateral hilar lymphadenopathy on chest radiograph (shown below). What could be the diagnosis?
In tuberculosis the cytokine causing fever is
Warthin-Finkeldey cells are seen in
Stellate granulomas are seen in
ABO non- secretors are more prone to ?
Primary complex of M bovis involves:
What does Ghon's focus indicate in the context of tuberculosis?
Practice by Chapter
Host-Pathogen Interactions
Practice Questions
Bacterial Infections
Practice Questions
Viral Infections
Practice Questions
Fungal Infections
Practice Questions
Parasitic Diseases
Practice Questions
Emerging Infections
Practice Questions
Healthcare-Associated Infections
Practice Questions
Infectious Disease Pathology in Immunocompromised Hosts
Practice Questions
Laboratory Diagnosis of Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app