
Infectious Diseases — MCQs

On this page
Which of the following is a difference between herpangina and primary herpetic stomatitis?
Foam cells are seen in infection with which virus?
Primary complex in which of the following sites suggests congenital tuberculosis?
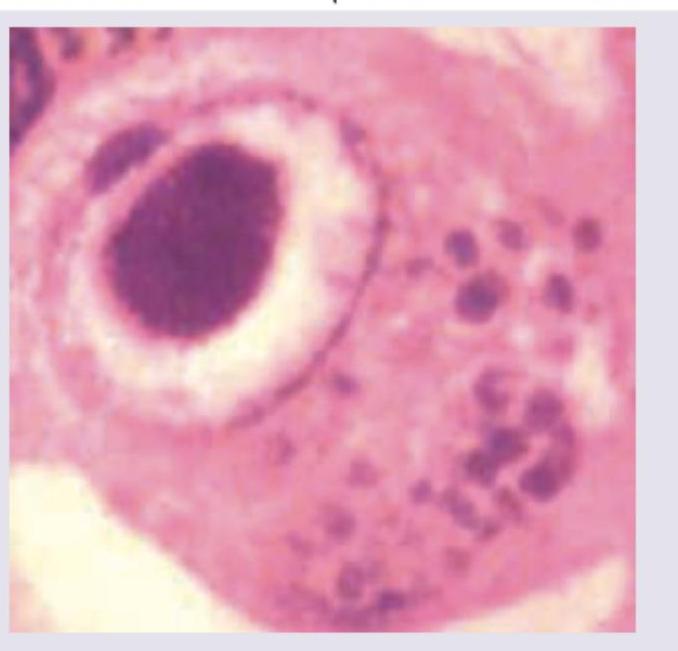
The given inclusion bodies are characteristic of which of the following organisms? 
Which is true about the inclusion bodies seen in specimen of patient, who underwent a liver transplantation?
The earliest specific cystoscopic appearance of Bilharzial cystitis is :
What is the primary reason for the development of granuloma formation in tertiary syphilis?
What mechanism explains the pathogenesis of Jarisch-Herxheimer reaction in patients treated for syphilis?
What is the main mechanism by which Treponema pallidum causes tissue damage in tertiary syphilis?
In lymphoid tissue biopsy from a patient with suspected measles, multinucleated giant cells with 'clockwise' nuclear arrangement are observed. What are these cells called?
Practice by Chapter
Host-Pathogen Interactions
Practice Questions
Bacterial Infections
Practice Questions
Viral Infections
Practice Questions
Fungal Infections
Practice Questions
Parasitic Diseases
Practice Questions
Emerging Infections
Practice Questions
Healthcare-Associated Infections
Practice Questions
Infectious Disease Pathology in Immunocompromised Hosts
Practice Questions
Laboratory Diagnosis of Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app