
Infectious Diseases — MCQs

On this page
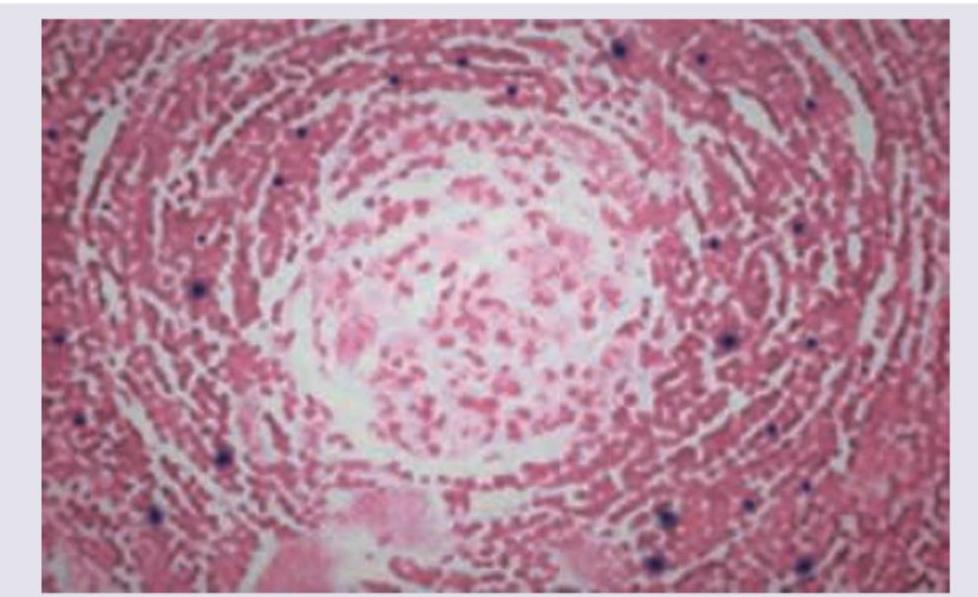
A 40-year-old man underwent lung transplantation. The resected lung specimen is shown below. Comment on the diagnosis.
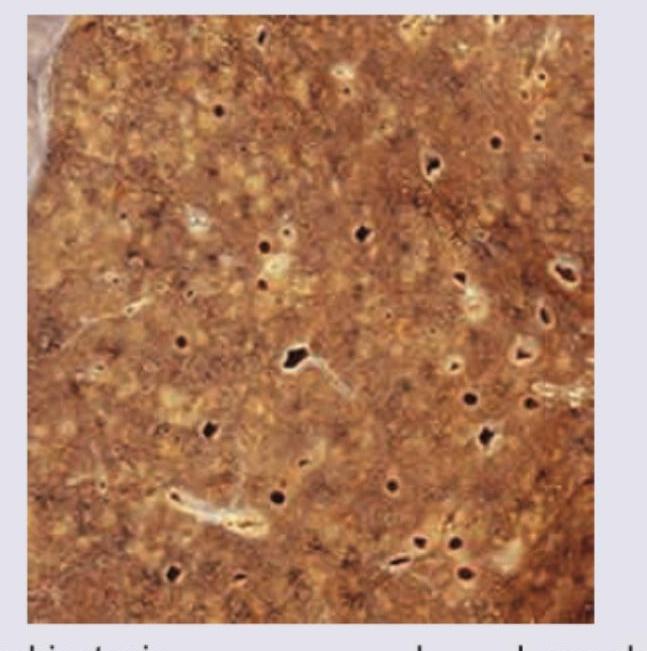
A patient presents with intermittent fever, no weight loss and enlarged retroperitoneal lymph nodes. Peripheral smear is normal. Gross sample and its histopathology slide is shown below. Comment on the diagnosis.
Which of the following tubes contain sodium fluoride as an anti-coagulant?
The earliest specific cystoscopic appearance of Bilharzial cystitis is :
"Collar-stud" abscess is seen in :
What is the primary reason for the development of granuloma formation in tertiary syphilis?
A 42 year-old female patient presents with cough, low-grade fever, and hemoptysis. Investigations reveal a cavitary lesion on her right lung apex, which on biopsy reveals caseous necrosis. The underlying pathophysiology is:
What is the mechanism by which Chlamydia trachomatis causes cellular damage in urethritis?
Cellulitis is characterized as:
Which of the following infectious diseases is the most likely cause of granuloma formation?
Practice by Chapter
Host-Pathogen Interactions
Practice Questions
Bacterial Infections
Practice Questions
Viral Infections
Practice Questions
Fungal Infections
Practice Questions
Parasitic Diseases
Practice Questions
Emerging Infections
Practice Questions
Healthcare-Associated Infections
Practice Questions
Infectious Disease Pathology in Immunocompromised Hosts
Practice Questions
Laboratory Diagnosis of Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app