
Infectious Diseases — MCQs

On this page
All the following malignancies are associated with HIV, except?
Which of the following is a difference between herpangina and primary herpetic stomatitis?
What is the best laboratory test for diagnosing Lupus vulgaris in the oral cavity?
What are the clinical features of infectious mononucleosis?
What is a tuberculoma?
A 25-year-old presents with painful vesicular lesions on the lips. A Tzanck smear from the lesion base shows multinucleated giant cells. What is the most likely causative agent?
The given inclusion bodies are characteristic of which of the following organisms? 
A male patient presents with fever, cough, and hemoptysis. Bronchoalveolar lavage (BAL) fluid examination shows septate hyphae with acute angle (dichotomous) branching under microscopy. What is the most likely diagnosis?
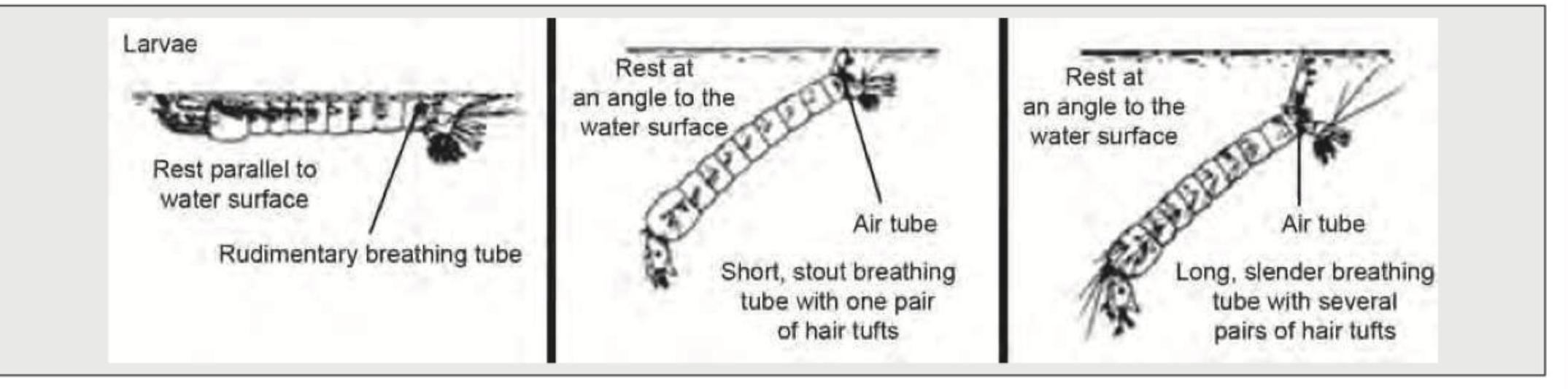
Identify the Anopheles mosquito larva from the image shown below:
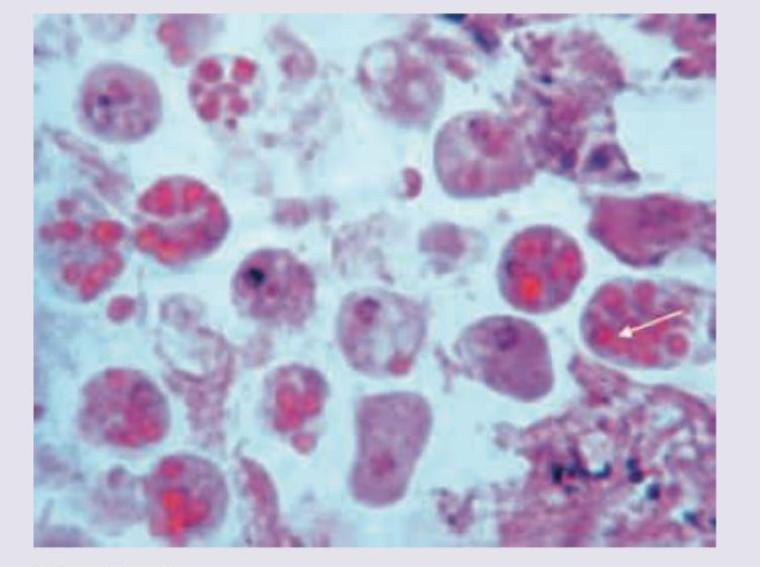
A 23-year-old male presented with abdominal pain and bloody diarrhea of one week duration. The following colonoscopic biopsy is diagnostic of infection with:
Practice by Chapter
Host-Pathogen Interactions
Practice Questions
Bacterial Infections
Practice Questions
Viral Infections
Practice Questions
Fungal Infections
Practice Questions
Parasitic Diseases
Practice Questions
Emerging Infections
Practice Questions
Healthcare-Associated Infections
Practice Questions
Infectious Disease Pathology in Immunocompromised Hosts
Practice Questions
Laboratory Diagnosis of Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app