
Infectious Diseases — MCQs

On this page
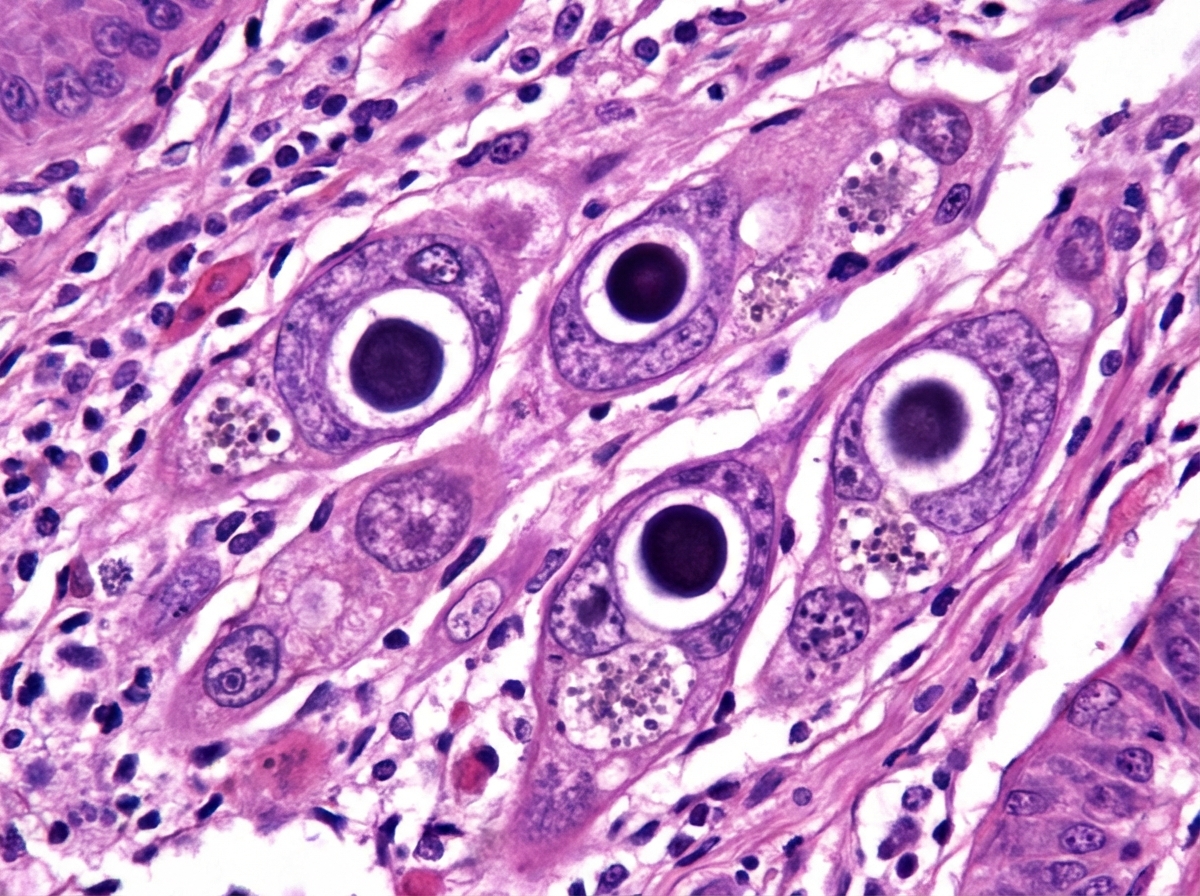
A 45-year-old HIV-positive male presented with dysphagia. Endoscopy and biopsy were performed. What is the most likely diagnosis based on the endoscopic and histological findings?
Which of the following is the brownish-colored substance seen in heart failure cells?
What is the multifocal tumor of vascular origin commonly seen in a patient with AIDS?
Hepatitis B virus (HBV) infection is associated with all of the following conditions except:
Erythrophagia and Mononuclear cell infiltration ulcers are seen in which condition?
In Tuberculosis, what type of cells primarily provide immunity?
A 37-year-old man presents with a productive cough, fever, and night sweats. A chest X-ray reveals an ill-defined area of consolidation at the periphery of the right middle lobe and mediastinal lymphadenopathy. Sputum culture is positive for acid-fast bacilli. What pathologic finding is most likely to be seen in a lymph node biopsy from this patient?
Which of the following statements is NOT TRUE regarding primary Herpes Simplex Virus (HSV) infections?
Which of the following is NOT a disease caused by coxsackievirus?
Which of the following statements regarding Viridans streptococci is TRUE?
Practice by Chapter
Host-Pathogen Interactions
Practice Questions
Bacterial Infections
Practice Questions
Viral Infections
Practice Questions
Fungal Infections
Practice Questions
Parasitic Diseases
Practice Questions
Emerging Infections
Practice Questions
Healthcare-Associated Infections
Practice Questions
Infectious Disease Pathology in Immunocompromised Hosts
Practice Questions
Laboratory Diagnosis of Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app