
Laboratory Diagnosis of Infections — MCQs

Arrange the following in sequential order with regards to the steps of collection of samples for pap smear testing: Use posterior vaginal wall retractor Take the sample Make smear on a slide Fix the smear
Which of the following molecular analysis methods is used to detect RNA?
A patient with prolonged ICU stay develops fever and hypotension. Blood culture shows budding yeast with pseudohyphae. What is the best rapid test to speciate this organism?
Blood culture is positive in which infection caused by Staphylococcus aureus?
A farmer presents to the emergency department with painful inguinal lymphadenopathy and a history of fever and flu-like symptoms. Clinical examination reveals an ulcer on the leg. Which of the following stains should be used to detect suspected bipolar-stained organisms?
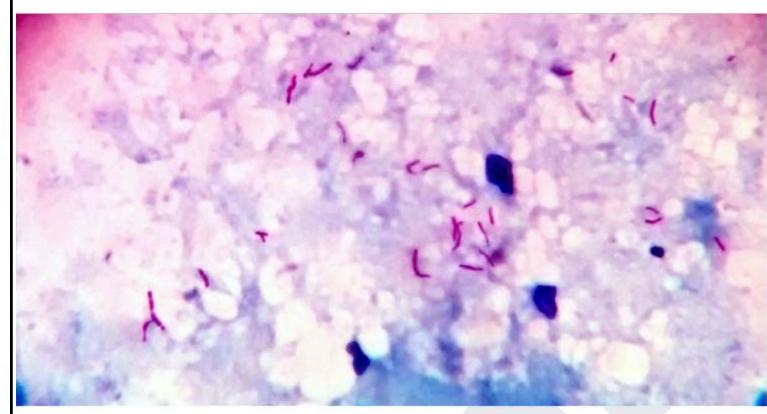
A 32 year old laborer working at a construction site presented with fever and hemoptysis. The sputum sample collected for examination showed the following. The smear will be stained by which of the following sequences?
What are the reasons a sample may be disqualified for culture?
Which of the following is true about anti-CMV IgG antibodies?
In a patient presenting with fever and suspected systemic infection, which of the following specimens is the most appropriate for the isolation of microorganisms in laboratory diagnosis?
What is the clinical significance of the Vi antigen in Salmonella typhi?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app