
Immunopathology — MCQs

On this page
Thymic hypoplasia is seen in which of the following conditions?
Which type of hypersensitivity reaction is Rh incompatibility?
Human leukocyte antigen (HLA), which plays an important role in graft rejection, is present on which chromosome?
SS-A (Ro) and SS-B (La) antibodies found in Sjogren syndrome are targeted against which cellular component?
All of the following are neoplasms found in patients with HIV infection EXCEPT?
Which pair of organs is involved in Goodpasture's syndrome?
Sago spleen is seen in which condition?
Granuloma formation is seen in which type of hypersensitivity reaction?
Which of the following is a type III hypersensitivity reaction?
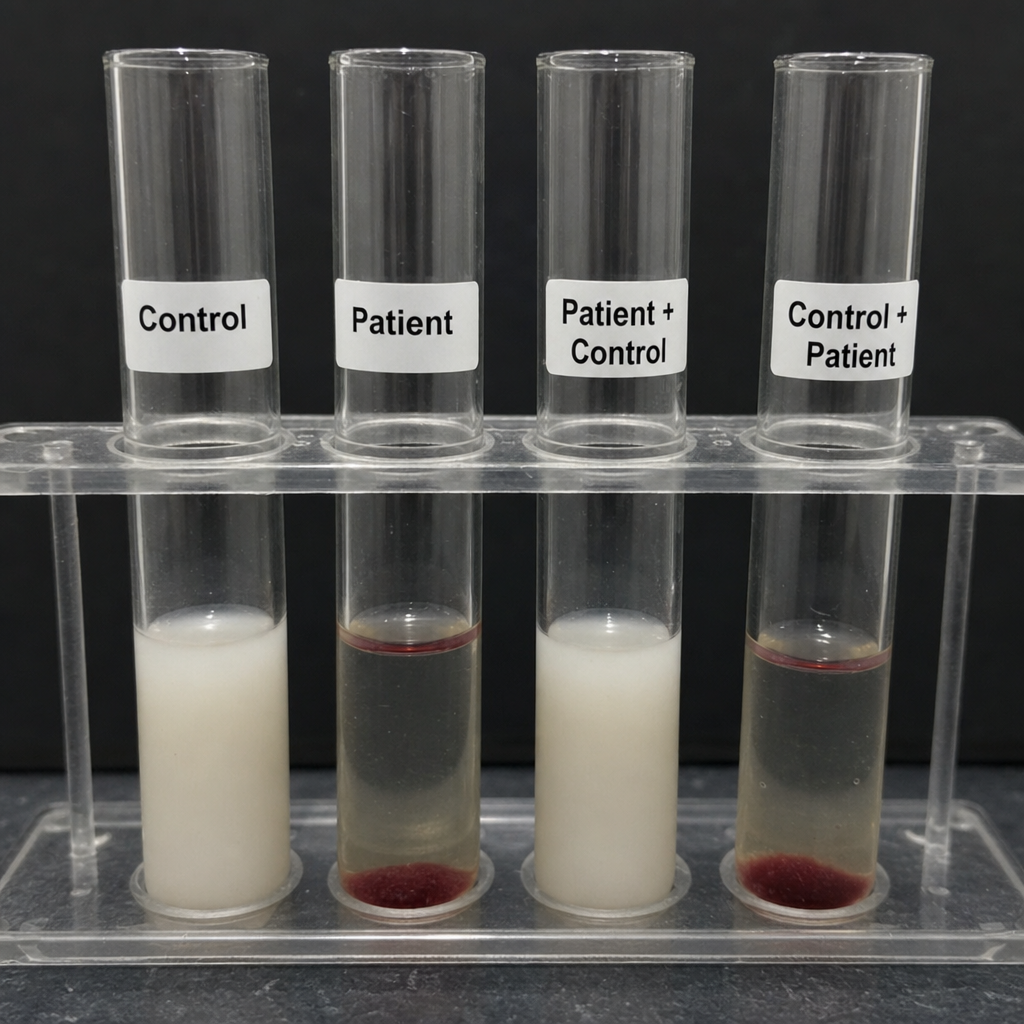
A 5-year-old boy presented with pyogenic abscess, runny nose, oral thrush & rash on perineal areas. On culturing pus Staphylococcus aureus was isolated. A test was performed whose finding is shown below. Which of the following is the most likely gene involved in the above condition?
Practice by Chapter
Cells and Tissues of the Immune System
Practice Questions
Innate Immunity
Practice Questions
Adaptive Immunity
Practice Questions
Hypersensitivity Reactions
Practice Questions
Autoimmune Diseases
Practice Questions
Immunodeficiency Disorders
Practice Questions
Transplantation Immunopathology
Practice Questions
Immune Response to Infections
Practice Questions
Immunologic Laboratory Techniques
Practice Questions
Tumor Immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app