
Immunopathology — MCQs

On this page
Antibody-dependent cell-mediated cytotoxicity (ADCC) is a mechanism by which target cells are killed. Which immune cells are primarily involved in ADCC?
Which type of cell mediates the immunological reaction against a transplanted organ?
Which CD molecule is important for the presentation of lipid antigens?
All are true regarding agammaglobulinemia except:
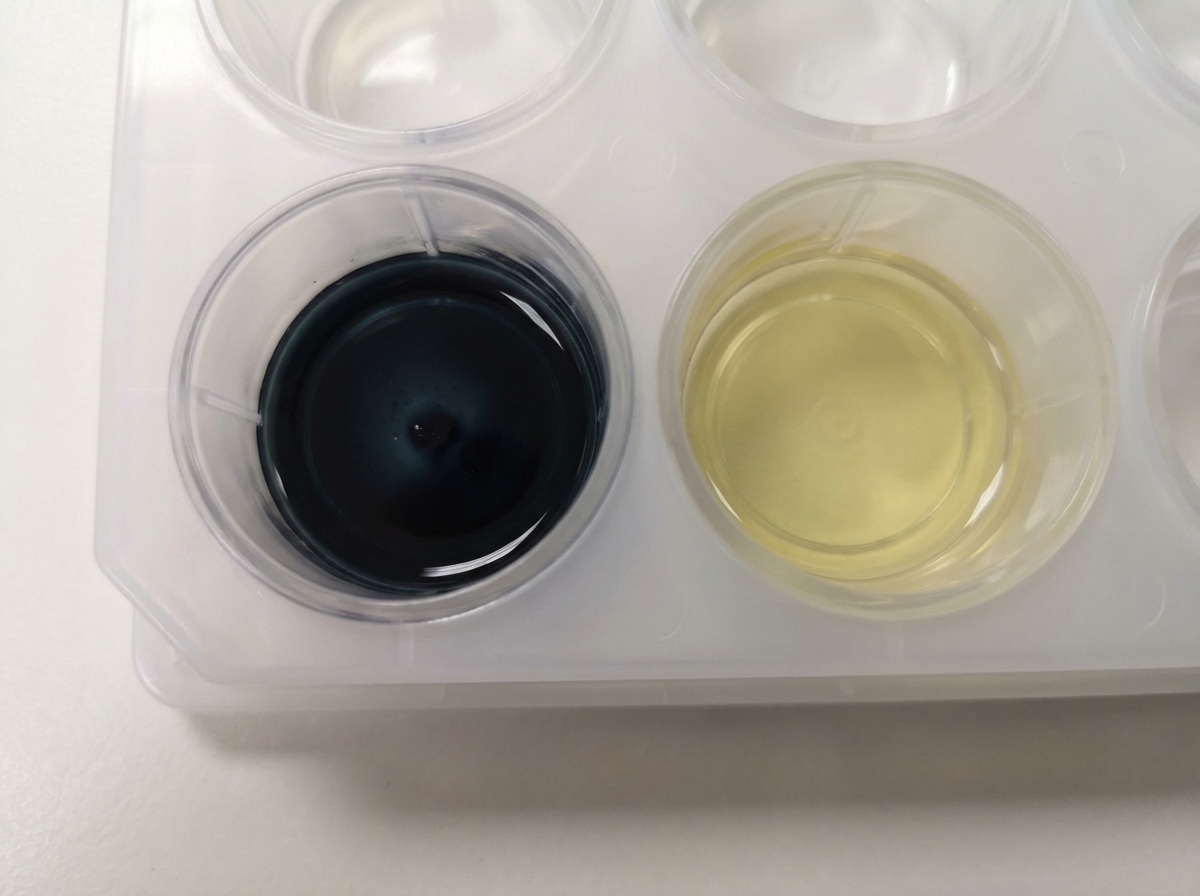
A 6-year-old boy presented with recurrent pyogenic abscess, runny nose, oral thrush, and rash on perineal areas. Pus culture showed growth of Staphylococcus aureus. A test was performed whose finding is shown below. What is the most common mode of inheritance of this disorder?
Which immunoglobulin (Ig) is primarily active in Type 1 hypersensitivity reactions?
All of the following are true regarding Bruton's Agammaglobulinemia except:
A 10-year-old boy with a history of recurrent bacterial infections presents with fever and a productive cough. Biochemical analysis of his neutrophils demonstrates defective oxidative burst. This patient most likely has inherited mutations in the gene that encodes which of the following proteins?
Which is the most important Human Leukocyte Antigen (HLA) locus for organ transplantation and tissue typing?
All of the following autoimmune disorders are more common in females, except:
Practice by Chapter
Cells and Tissues of the Immune System
Practice Questions
Innate Immunity
Practice Questions
Adaptive Immunity
Practice Questions
Hypersensitivity Reactions
Practice Questions
Autoimmune Diseases
Practice Questions
Immunodeficiency Disorders
Practice Questions
Transplantation Immunopathology
Practice Questions
Immune Response to Infections
Practice Questions
Immunologic Laboratory Techniques
Practice Questions
Tumor Immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app