
Immunopathology — MCQs

On this page
Which of the following is NOT a feature of DiGeorge Syndrome?
All of the following immunodeficiency diseases are due to chromosomal instability or defective repair of genes, except:
Which antigen is primarily involved in post-transplant rejection?
Thymoma is associated with which of the following conditions?
Which of the following organs can cause an antigen reaction when exposed in self-blood?
An 8-month-old boy is evaluated because of repeated episodes of pneumococcal pneumonia. Serum studies demonstrate very low levels of IgM, IgG, and IgA. This patient's condition is related to a deficiency of which of the following proteins?
Hematoxylin bodies are seen in which of the following conditions?
A 27-year-old male patient with blood group O presents with massive intestinal bleeding and has lost half his blood volume. He is transfused with blood group AB blood. Within minutes, he develops fever, chills, dyspnea, and a dramatic drop in blood pressure. What is the most likely cause of this reaction?
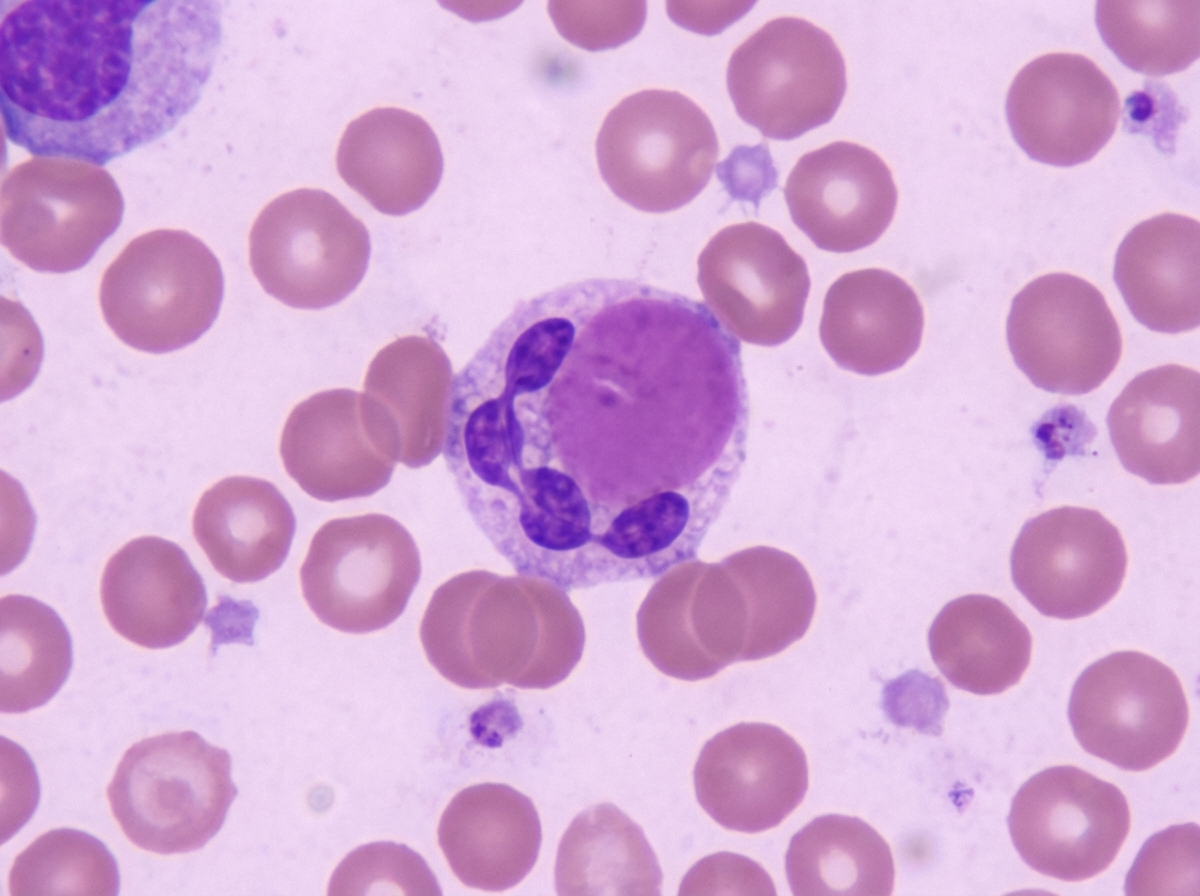
The image shows a cellular finding in a peripheral blood smear. This finding is most characteristic of which condition?
A 12-year-old boy presents with a 5-day history of sore throat. His temperature is 38.7°C (103°F). Physical examination reveals inflamed tonsils and swollen cervical lymph nodes. Trafficking and recirculation of blood-borne lymphocytes through the cervical lymph nodes in this patient occurs primarily at which of the following locations?
Practice by Chapter
Cells and Tissues of the Immune System
Practice Questions
Innate Immunity
Practice Questions
Adaptive Immunity
Practice Questions
Hypersensitivity Reactions
Practice Questions
Autoimmune Diseases
Practice Questions
Immunodeficiency Disorders
Practice Questions
Transplantation Immunopathology
Practice Questions
Immune Response to Infections
Practice Questions
Immunologic Laboratory Techniques
Practice Questions
Tumor Immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app