
Immunopathology — MCQs

On this page
Nude mice are able to accept xenografts because they lack which type of immune cell?
All of the following statements about Ataxia-Telangiectasia are true, except?
What is the distinguishing characteristic of a positive delayed-type hypersensitivity skin test?
In familial Mediterranean fever, which protein undergoes mutation?
The immediate type of hypersensitivity in which histamine does not play a major role is:
Epithelial granuloma is caused by which of the following?
Pinch purpura is seen in which of the following conditions?
What is the most common tumor associated with AIDS?
A 24-year-old man is infected with HIV during a sexual encounter. During the asymptomatic latent phase of his infection, the virus is actively proliferating and can be found in association with which of the following?
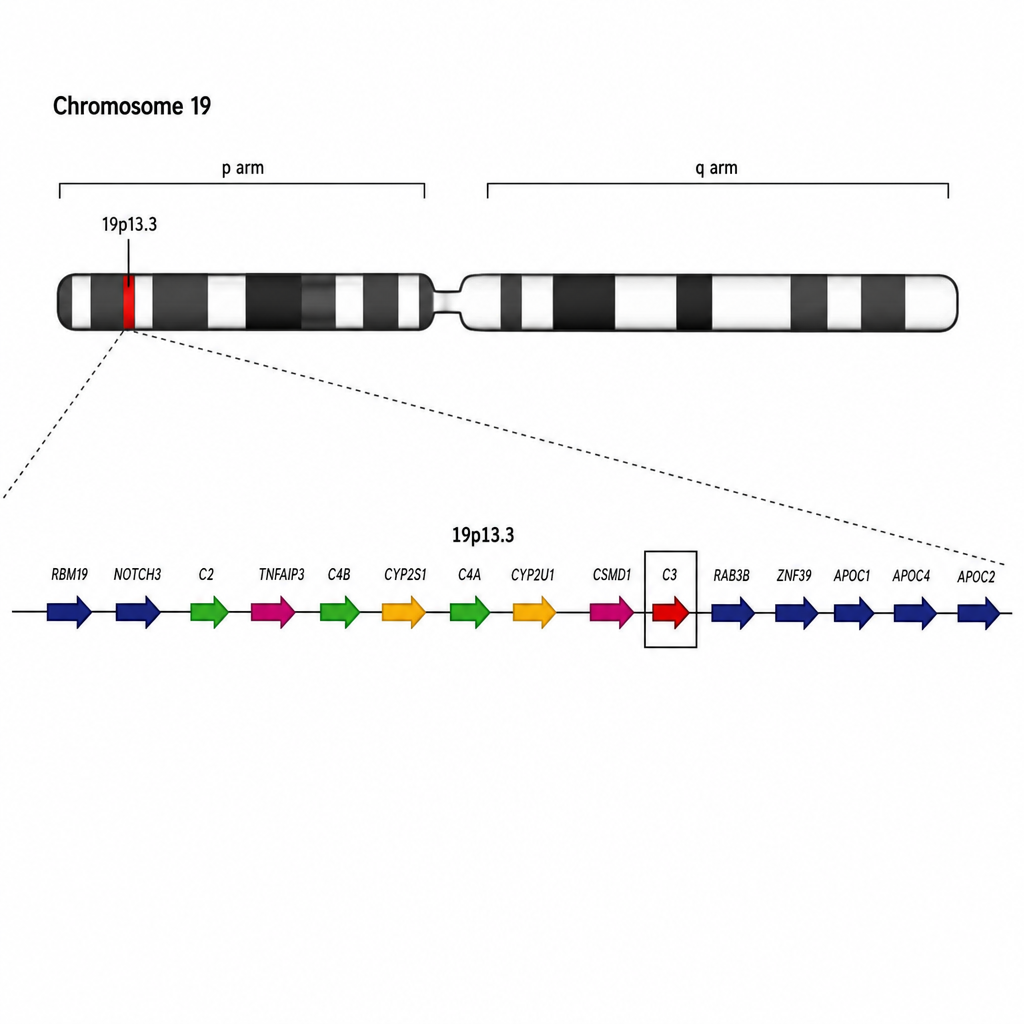
Which complement component is encoded by the given site?
Practice by Chapter
Cells and Tissues of the Immune System
Practice Questions
Innate Immunity
Practice Questions
Adaptive Immunity
Practice Questions
Hypersensitivity Reactions
Practice Questions
Autoimmune Diseases
Practice Questions
Immunodeficiency Disorders
Practice Questions
Transplantation Immunopathology
Practice Questions
Immune Response to Infections
Practice Questions
Immunologic Laboratory Techniques
Practice Questions
Tumor Immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app