
Hematopathology — MCQs

On this page
Presence of >10% plasma cells with no lytic lesion and M protein in serum is seen in?
Fragmented RBCs, sliced by fibrin bands, seen in intravascular hemolysis, are known as which of the following?
P.N.H is associated with all of the following conditions, except?
The HAM test is used to assess for which of the following?
Which of the following are the histological features of classical Hodgkin's disease?
What is the most common cause of complications in blood transfusion?
A 20-year-old carpenter presents with an enlarged and tender lymph node in the axilla due to a wound infection on his left thumb. A lymph node biopsy shows follicular enlargement and hyperemia, with sinuses filled with neutrophils. What is the most likely diagnosis?
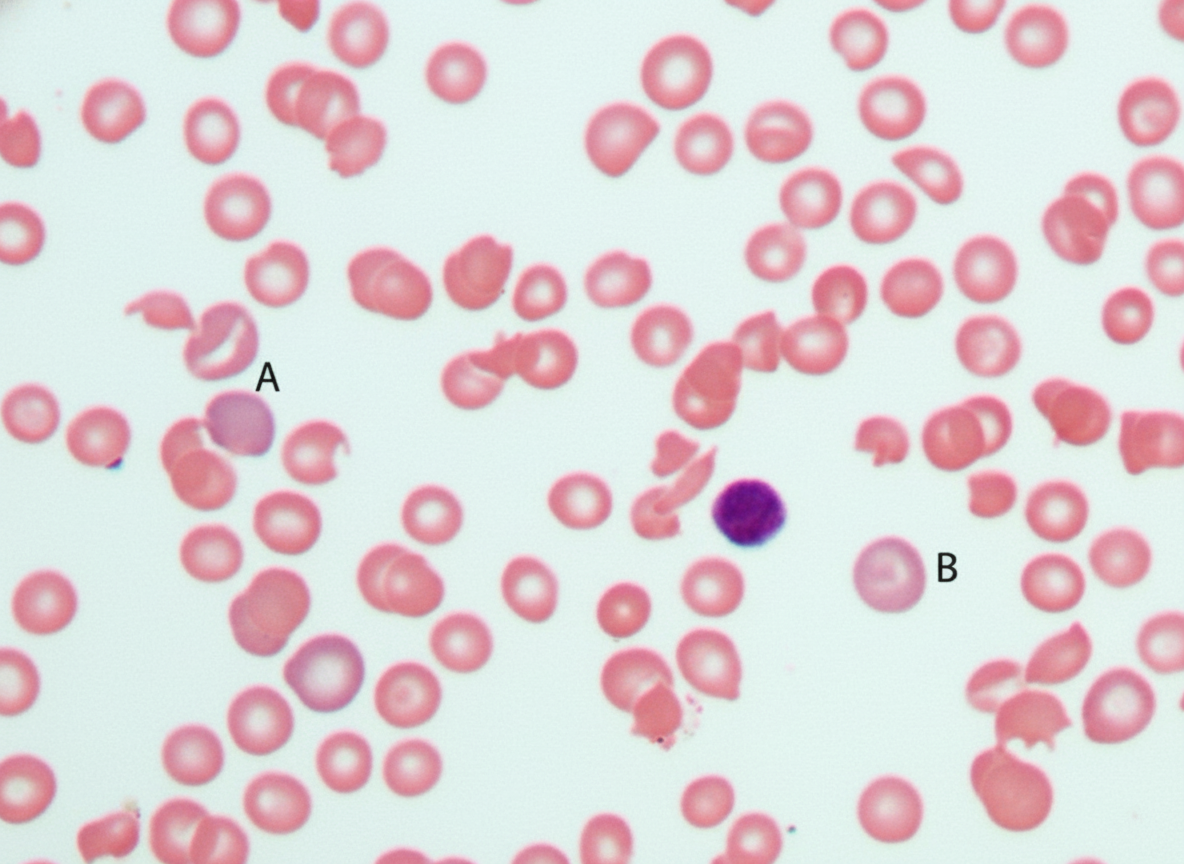
A 27-year-old black man develops sudden intravascular hemolysis 2 days after receiving the antimalarial drug primaquine, resulting in a decreased hematocrit, hemoglobinemia, and hemoglobinuria. Examination of the peripheral blood film is given. What is the most likely diagnosis?
All of the following are true regarding Von Willebrand's disease EXCEPT:
A 56-year-old male presents with low back pain, weight loss, fatigue, and recurrent sinus infections. He has no history of trauma. Examination reveals focal tenderness at the T10 level. Laboratory investigations show Hb of 9 g/dl and deranged renal function tests. A skull X-ray was performed. Bone marrow biopsy and serum protein electrophoresis are planned. What is the characteristic abnormality expected on the peripheral blood film?
Practice by Chapter
Anemias: Classification and Approach
Practice Questions
Hemolytic Anemias
Practice Questions
Myeloproliferative Neoplasms
Practice Questions
Myelodysplastic Syndromes
Practice Questions
Acute Leukemias
Practice Questions
Chronic Leukemias
Practice Questions
Lymphomas and Lymphoid Neoplasms
Practice Questions
Plasma Cell Disorders
Practice Questions
Bleeding Disorders
Practice Questions
Thrombotic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app