
Hematopathology — MCQs

On this page
Blast crises in Chronic Myeloid Leukemia (CML) are characterized by which of the following?
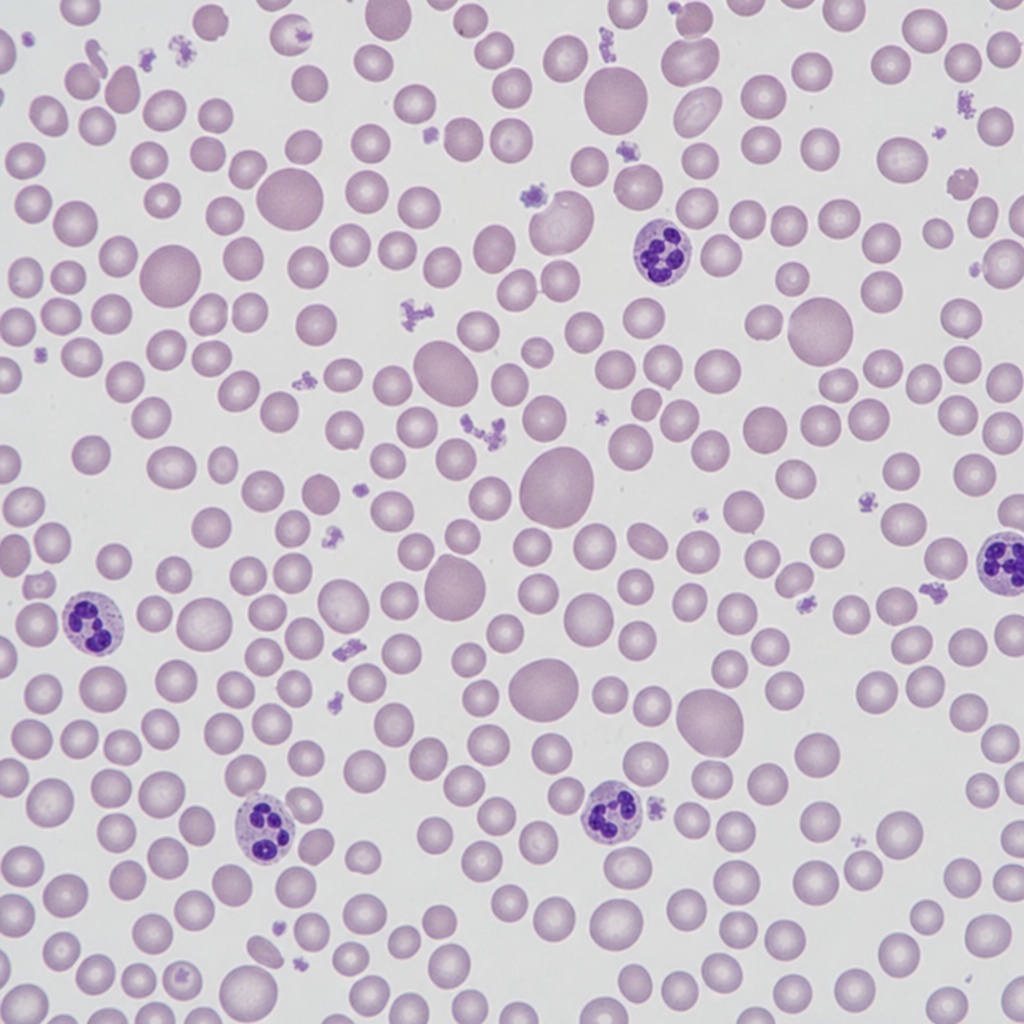
Comment on the type of anemia observed in a peripheral smear.
Acanthocytosis on peripheral smear is a feature of which of the following conditions?
Bence Jones proteins are composed of?
A 20-year-old female presented with complaints of easy bruising, frequent episodes of nose bleed, menorrhagia, and few episodes of upper gastrointestinal bleeding. On examination, purpura and petechial rash were noted. Laboratory findings revealed thrombocytopenia, normal prothrombin time (PT), and normal activated partial thromboplastin time (aPTT). Platelets do not aggregate in response to ristocetin after adding normal plasma, but have normal aggregation in response to adenosine diphosphate, epinephrine, and collagen. Platelet granules are normal. What is the most likely diagnosis in the above patient?
Which virus is known to cause hemopoietic carcinoma?
Which of the following conditions does NOT cause a prolonged PTT?
The direct globulin test is positive in which of the following conditions?
Which of the following statements is NOT true regarding idiopathic thrombocytopenic purpura?
After an accident, a male patient presented for routine evaluation. His RBCs showed Cabot's rings. What is the likely condition responsible?
Practice by Chapter
Anemias: Classification and Approach
Practice Questions
Hemolytic Anemias
Practice Questions
Myeloproliferative Neoplasms
Practice Questions
Myelodysplastic Syndromes
Practice Questions
Acute Leukemias
Practice Questions
Chronic Leukemias
Practice Questions
Lymphomas and Lymphoid Neoplasms
Practice Questions
Plasma Cell Disorders
Practice Questions
Bleeding Disorders
Practice Questions
Thrombotic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app