
Hematopathology — MCQs

On this page
All of the following are features of juvenile chronic myeloid leukemia except one.
A 50-year-old woman is discovered to have metastatic breast cancer and develops bacterial pneumonia one week after receiving her first dose of chemotherapy. Which of the following best explains this patient's susceptibility to bacterial infection?
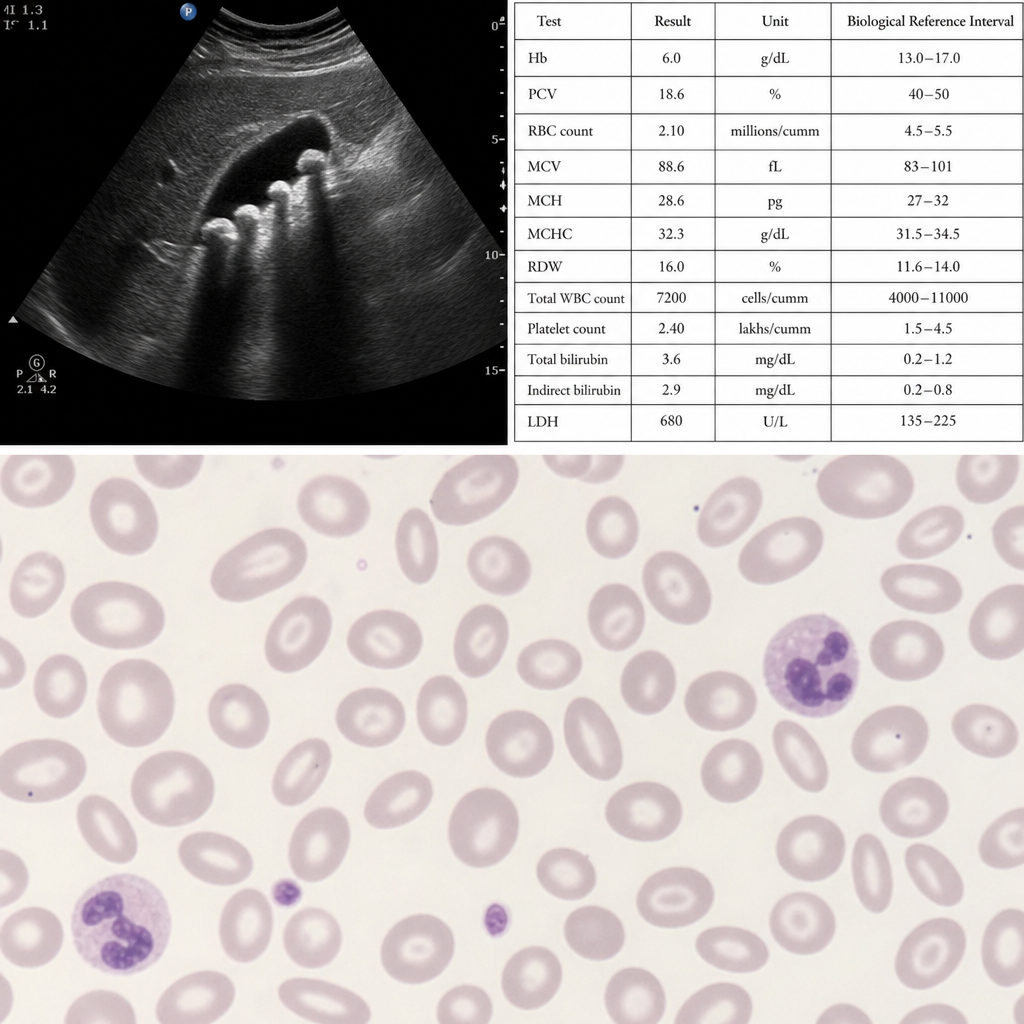
A 15-year-old boy presented with anemia and jaundice. On examination, his hemoglobin was 6 g/dL, ultrasound showed gallstones, and the peripheral smear showed the following. What is the most likely diagnosis?
Which of the following immunophenotypic features is characteristic of mantle cell lymphoma?
Which parameter is primarily used to diagnose macrocytosis in a complete blood count (CBC)?
Lethal midline granuloma arises from which cell type?
A 22-year-old woman presents with painless cervical lymphadenopathy, night sweats, and generalized pruritus. An enlarged cervical lymph node is removed for diagnosis, which shows broad bands of fibrosis on cut surface and histologically contains a mixture of cells, including lymphocytes, histiocytes, eosinophils, plasma cells, and scattered large cells with prominent nucleoli. Which of the following is the most likely condition?
What is the most effective method to prevent transfusion-associated graft-versus-host disease?
Flow cytometry is best used in the measurement of:
What is the most common type of acute myeloid leukemia in patients with Down's syndrome?
Practice by Chapter
Anemias: Classification and Approach
Practice Questions
Hemolytic Anemias
Practice Questions
Myeloproliferative Neoplasms
Practice Questions
Myelodysplastic Syndromes
Practice Questions
Acute Leukemias
Practice Questions
Chronic Leukemias
Practice Questions
Lymphomas and Lymphoid Neoplasms
Practice Questions
Plasma Cell Disorders
Practice Questions
Bleeding Disorders
Practice Questions
Thrombotic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app