
Hematopathology — MCQs

On this page
Blood is stored at what temperature in blood bank?
What is the defect in Glanzmann's thrombasthenia?
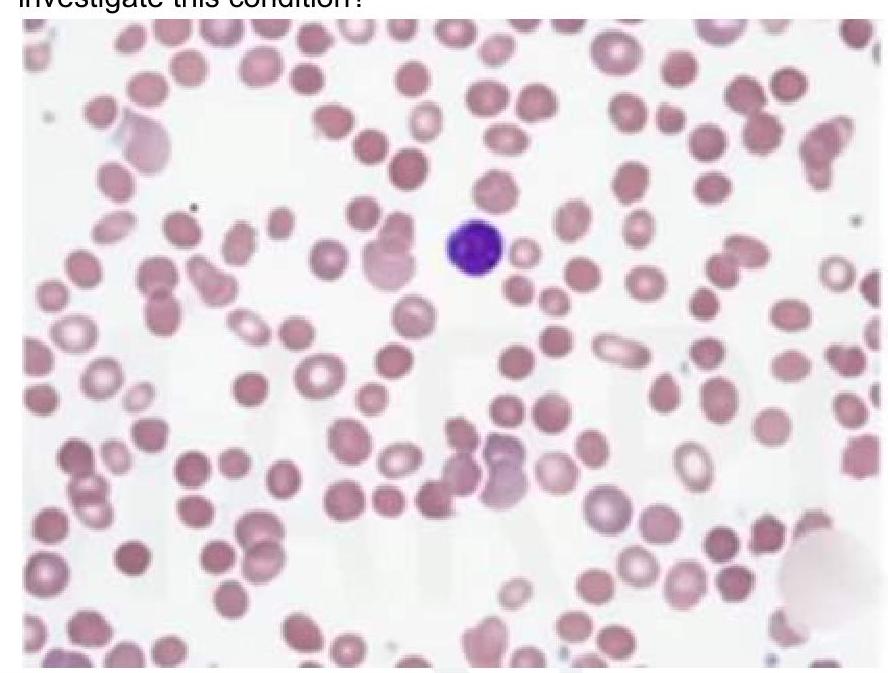
A child presents with intermittent jaundice and splenomegaly. There is a history of similar complaints in the elder brother. Peripheral smear shows the following finding. What is the most appropriate investigation for this condition?
A child presents with recurrent chest infections and abdominal pain. There is a history of 1 blood transfusion in the past. On examination, he had icterus and mild splenomegaly. Electrophoresis shows increased HbA2, HbF, and S spike. What is the likely diagnosis?
All trans retinoic acid is used in the treatment of acute promyelocytic leukemia (APL) associated with which genetic mutation?
In which type of Hodgkin's lymphoma are classical Reed-Sternberg cells most characteristically observed?
Which disease is associated with the CD59 marker?
TRALI occurs within how many hours of transfusion?
Whole blood is used as a sample for which test?
Bernard–Soulier syndrome is caused by a deficiency of which glycoprotein complex?
Practice by Chapter
Anemias: Classification and Approach
Practice Questions
Hemolytic Anemias
Practice Questions
Myeloproliferative Neoplasms
Practice Questions
Myelodysplastic Syndromes
Practice Questions
Acute Leukemias
Practice Questions
Chronic Leukemias
Practice Questions
Lymphomas and Lymphoid Neoplasms
Practice Questions
Plasma Cell Disorders
Practice Questions
Bleeding Disorders
Practice Questions
Thrombotic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app