
Hematopathology — MCQs

On this page
The image shows:
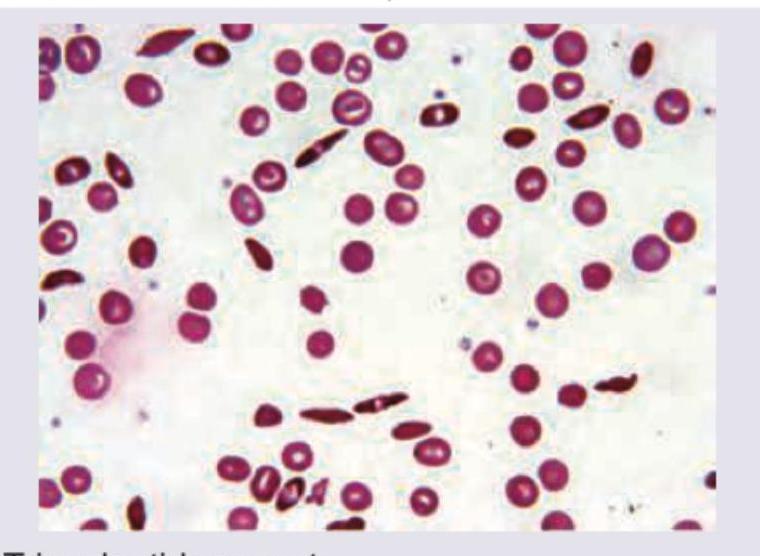
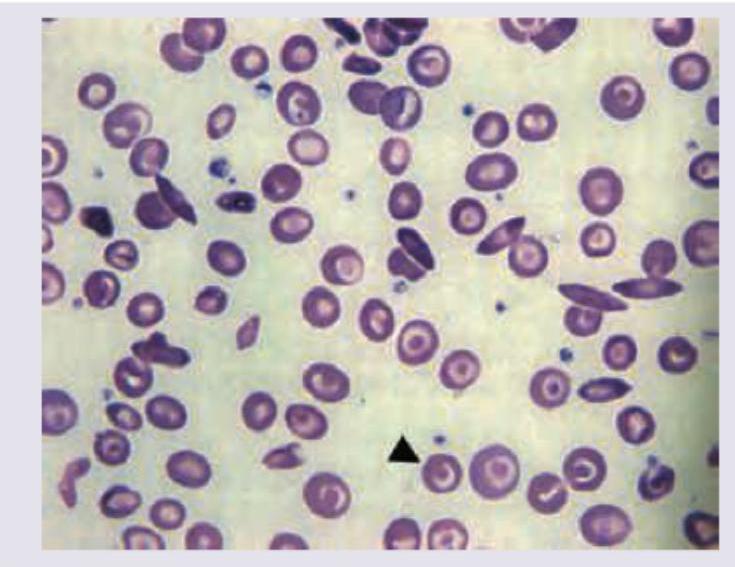
A 6-year-old Afro-American boy presents with acute abdomen and nonhealing ulcer on medial malleolus. Peripheral smear is shown. The most likely cause of this condition is:
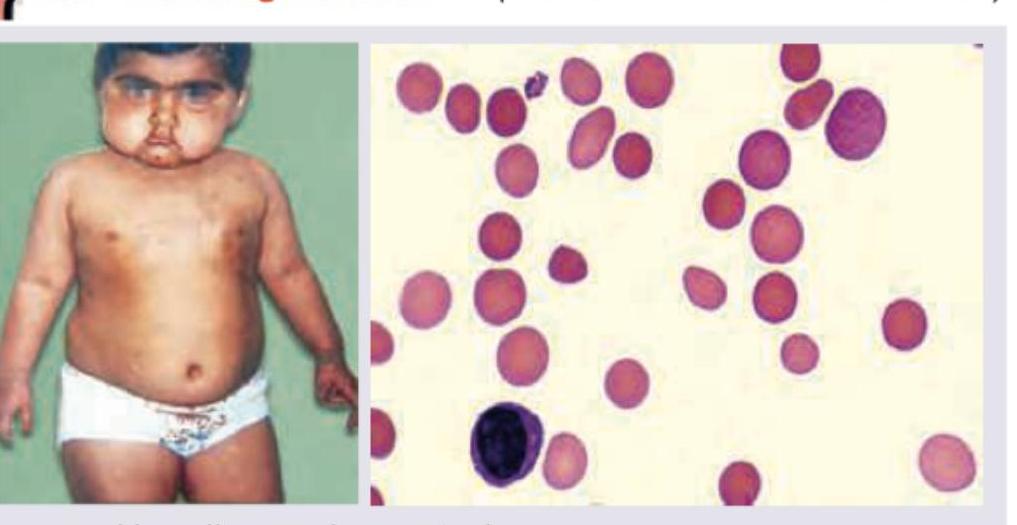
A 16-year-old female with pallor and hepatosplenomegaly presents to your clinic. She has a history of chronic anemia not requiring regular blood transfusions, and hemoglobin electrophoresis shows elevated HbA2 and HbF with reduced HbA. Peripheral smear shows:
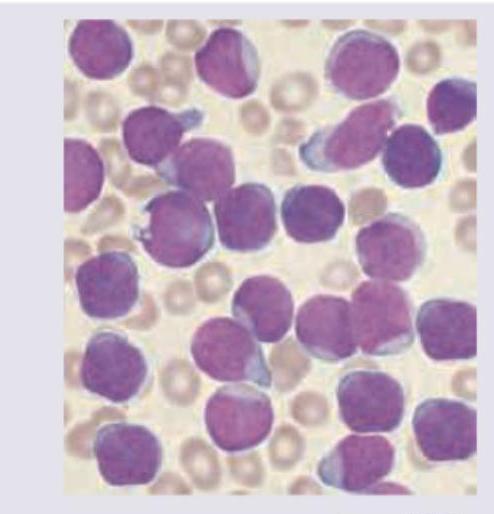
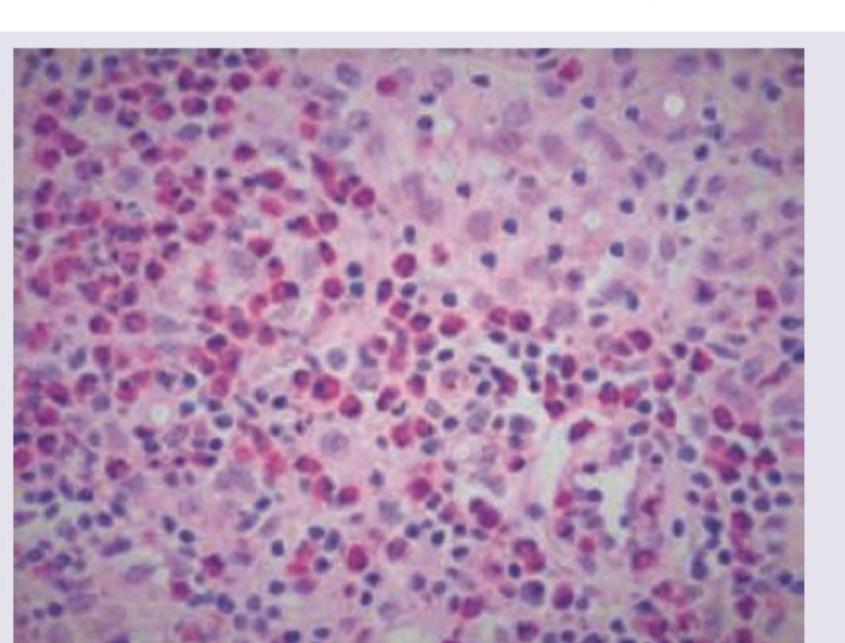
A 7-year-old boy presents with fever and weight loss. On examination he had pallor with lymphadenopathy. Peripheral smear is shown below. Diagnosis is: (AIIMS May 2017)
A patient presents with a solitary bone lesion. Histopathological examination shows the following microscopic features. What is the most likely diagnosis?
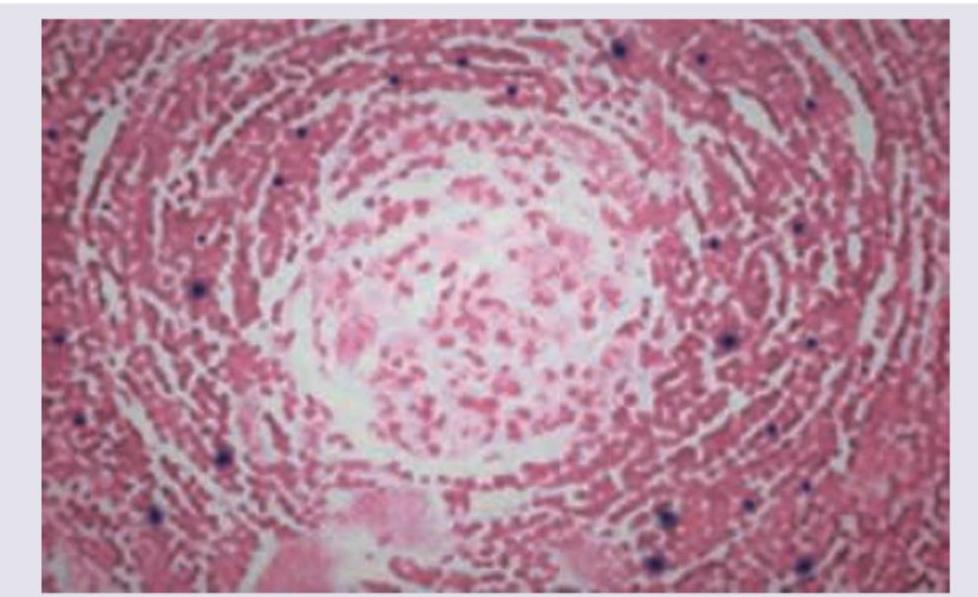
A patient presents with intermittent fever, no weight loss and a single enlarged retroperitoneal lymph node. Peripheral smear is normal. Gross sample and its histopathology slide is shown below. Comment on the diagnosis.
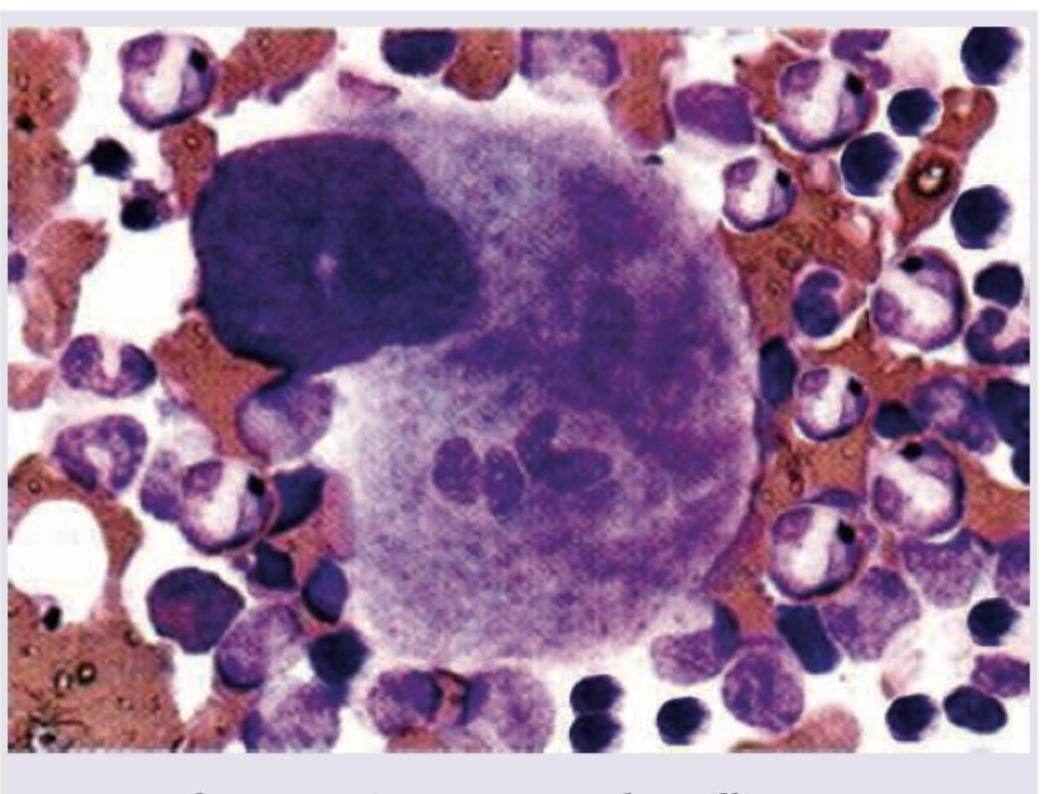
A megakaryocyte contains intact hematopoietic cells as shown in the image; this phenomenon is known as?
Which of the following hematological findings are seen in pregnant women with thalassemia trait?
Which of the following are metabolic causes of splenic enlargement?
Folic acid deficiency is characterized by the following features except
Practice by Chapter
Anemias: Classification and Approach
Practice Questions
Hemolytic Anemias
Practice Questions
Myeloproliferative Neoplasms
Practice Questions
Myelodysplastic Syndromes
Practice Questions
Acute Leukemias
Practice Questions
Chronic Leukemias
Practice Questions
Lymphomas and Lymphoid Neoplasms
Practice Questions
Plasma Cell Disorders
Practice Questions
Bleeding Disorders
Practice Questions
Thrombotic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app