
Hematopathology — MCQs

On this page
Which of the following is the most common chromosomal abnormality associated with acute myeloid leukemia (AML) with a favorable prognosis?
A 68-year-old man presents with bleeding manifestations. Peripheral smear shows the presence of cells shown below. Which of the following is the most common chromosomal abnormality seen in this condition?
Which of the following laboratory techniques is most commonly used to compare and quantify CD markers on cells?
A lymphoma characterized by the presence of centrocytes and centroblasts, along with BCL2 positivity and CD10 expression, is most commonly associated with which chromosomal translocation?
The following image shows:

The following test is performed for which condition?
A 3-year-old child presents with bleeding from nose and Periorbital Ecchymosis. Sternal tenderness and bone pain is present. Peripheral smear shows presence of fragmented RBC and helmet cells. The most probable diagnosis is? (Recent NEET Pattern 2016-17)
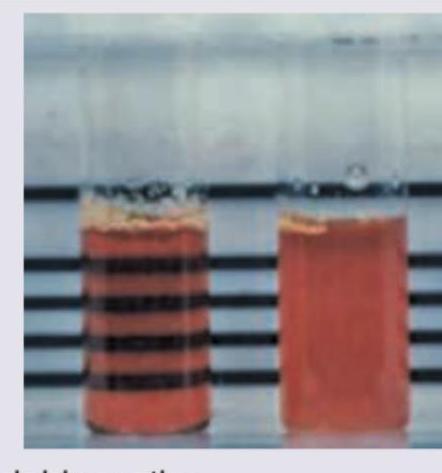
All are true about the blood component shown below except?

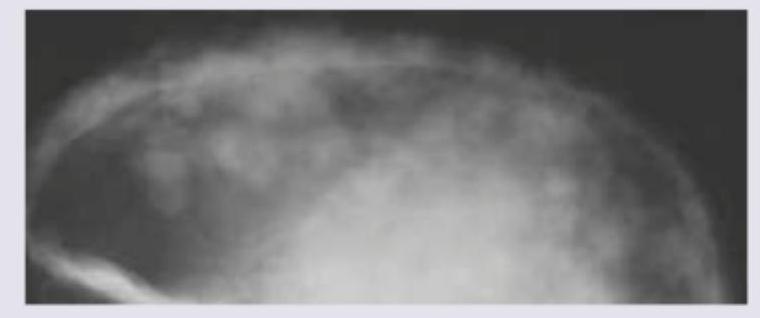
A 6-year-old child presents with a painful scalp swelling and mild fever. The skull X-ray is shown below. Which of the following will be the most probable diagnostic finding in this patient?
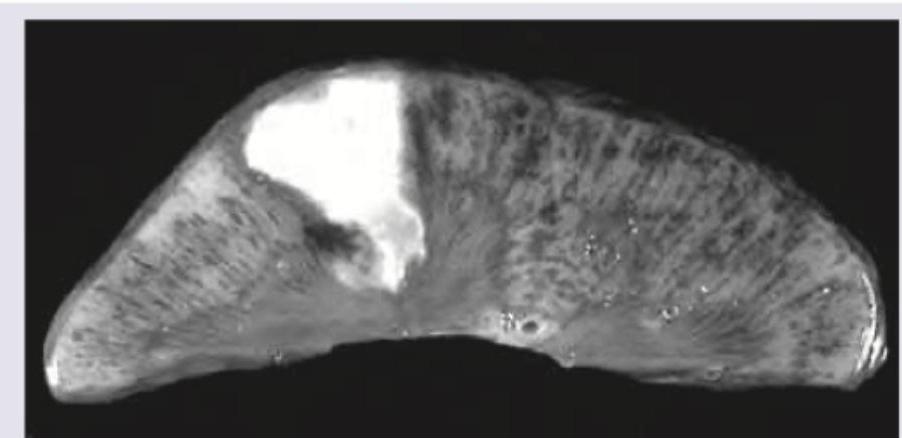
A 10-year-old Sindhi boy presents with recurrent episodes of bone pain. Specimen shows:
Practice by Chapter
Anemias: Classification and Approach
Practice Questions
Hemolytic Anemias
Practice Questions
Myeloproliferative Neoplasms
Practice Questions
Myelodysplastic Syndromes
Practice Questions
Acute Leukemias
Practice Questions
Chronic Leukemias
Practice Questions
Lymphomas and Lymphoid Neoplasms
Practice Questions
Plasma Cell Disorders
Practice Questions
Bleeding Disorders
Practice Questions
Thrombotic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app