
Hematopathology — MCQs

On this page
Pancytopenia with hypercellular marrow may be seen due to all of the following except:
Aplastic anemia is characterized by which of the following findings?
Which of the following are types of Hodgkin's lymphoma?
A 36-year-old male presents with weakness, pallor, and bleeding gums. His HB was 7 g/dL, total leukocyte count was 110,000/mm³ with many immature white blood cells positive for MPO, and platelet count was 22,000/mm³. What is the most likely diagnosis?
Iron deficiency is best demonstrated by?
Microangiopathic hemolytic anemia (MAHA) is a component of all of the following, except?
Bence Jones proteinuria is found on a urinalysis specimen from a 63-year-old woman who is developing chronic renal failure with high serum urea nitrogen and creatinine. A radiograph of the vertebral column demonstrates multiple 1 to 2 cm rounded areas of decreased bone density. The pathological examination from a renal biopsy is likely to show which of the following complications?
A patient presents with a lytic bone lesion. Histology reveals monoclonal plasma cells. Bone marrow biopsy shows less than 10 percent plasma cells, and a small M spike is reported on electrophoresis. Skeletal survey is otherwise unremarkable. What is the most likely diagnosis?
Platelets can be stored at what temperature and for how long?
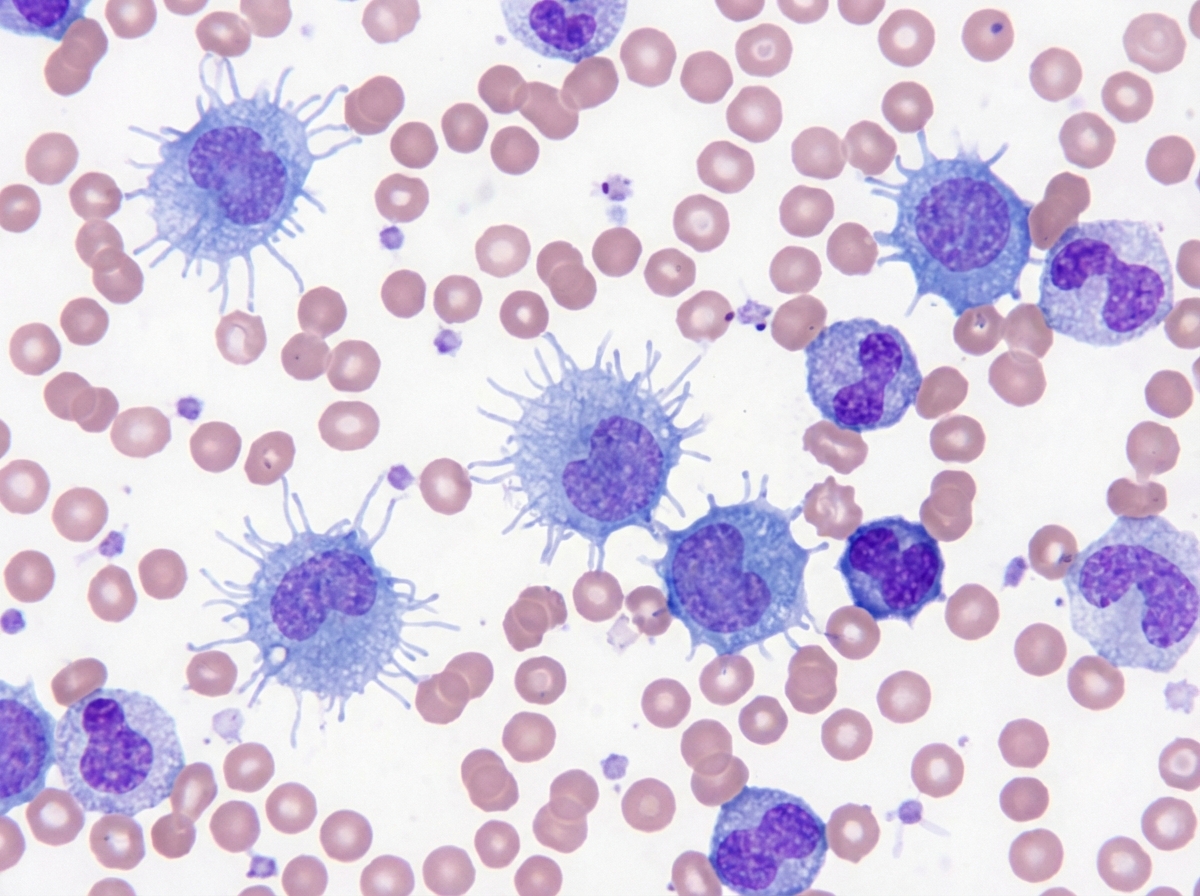
A 50-year-old male presented with left upper quadrant pain. On examination, the spleen was palpable 10 cm below the left costal margin. A peripheral smear is shown. Which of the following is the most specific immunohistochemical marker for classic hairy cell leukemia?
Practice by Chapter
Anemias: Classification and Approach
Practice Questions
Hemolytic Anemias
Practice Questions
Myeloproliferative Neoplasms
Practice Questions
Myelodysplastic Syndromes
Practice Questions
Acute Leukemias
Practice Questions
Chronic Leukemias
Practice Questions
Lymphomas and Lymphoid Neoplasms
Practice Questions
Plasma Cell Disorders
Practice Questions
Bleeding Disorders
Practice Questions
Thrombotic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app