
General Pathology — MCQs

On this page
Fat necrosis is common in:
White infarcts are seen in which of the following?
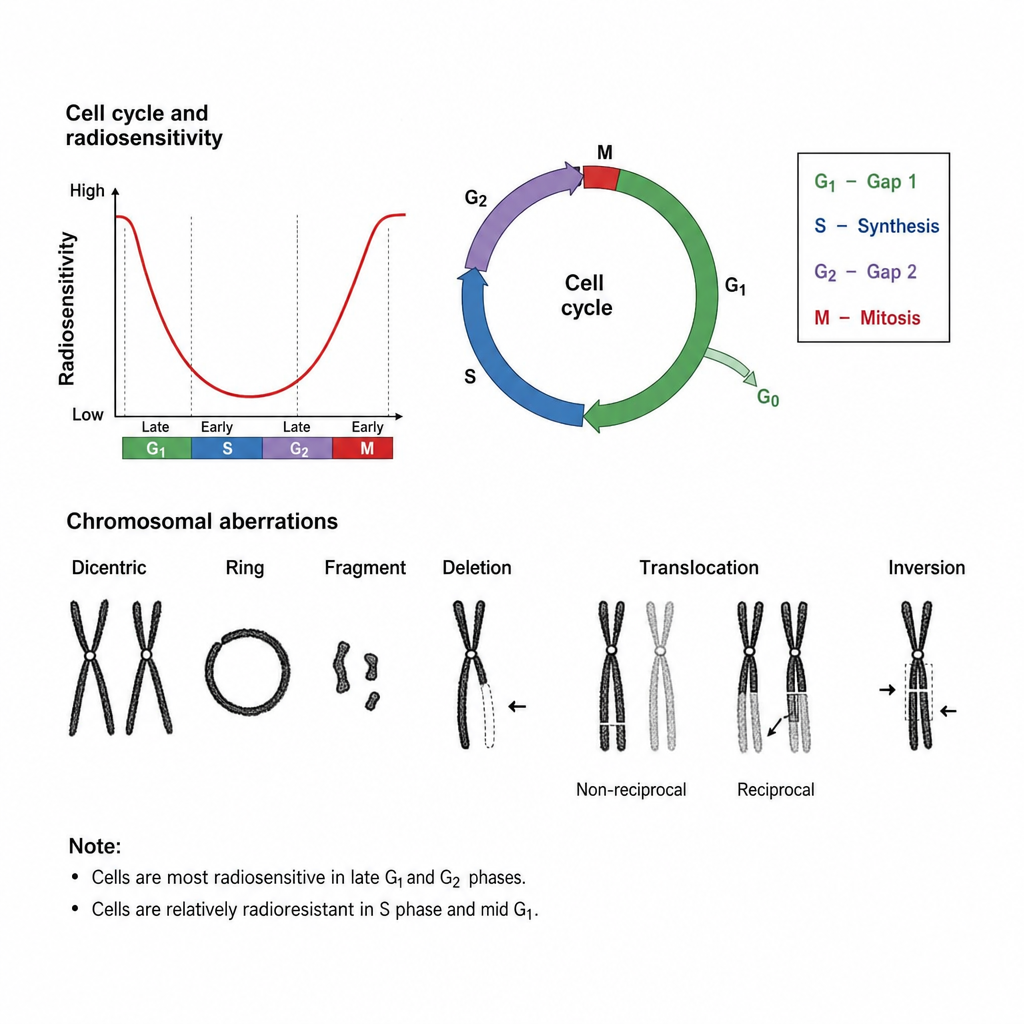
Which of these cells is most radio-resistant?
Which of the following is an anti-apoptotic gene?
Which of the following is most susceptible to ionizing radiation?
The image below shows a chromosome-type aberration in which both sister chromatids display the same damage pattern (e.g., a dicentric chromosome). At which phase of the cell cycle did irradiation most likely occur to produce this pattern?
Type of necrosis seen in case of burn:
Crumpled paper appearance of cells is a feature of-
Stain used in electron microscopy
Endotoxin shock is initiated by:
Practice by Chapter
Cell Injury and Cell Death
Practice Questions
Adaptations of Cellular Growth
Practice Questions
Accumulations and Deposits
Practice Questions
Acute and Chronic Inflammation
Practice Questions
Tissue Repair and Wound Healing
Practice Questions
Hemodynamic Disorders
Practice Questions
Genetic Disorders
Practice Questions
Environmental Pathology
Practice Questions
Nutritional Diseases
Practice Questions
Molecular Basis of Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app