
General Pathology — MCQs

On this page
Caspase-1 mediated cell death with inflammation is known as
A middle-aged man from an endemic region presents with progressive swelling of the lower limb. A peripheral blood smear shows the following structure. What is the most likely cause of his limb swelling?
Which of the following types of cell death involves activation of caspase enzymes?
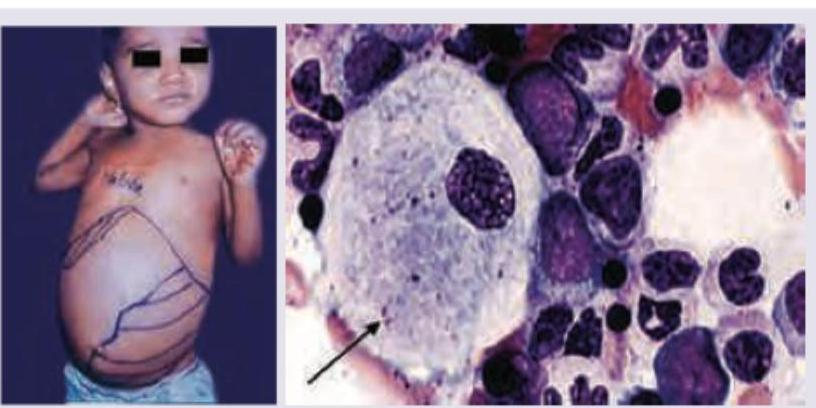
A 2-year-old child presents with growth retardation, pallor, bruising and has palpable spleen 5 cm below left costal margin. Bone marrow examination is shown below. Which is incorrect about the clinical diagnosis? (Recent NEET Pattern 2016-17)
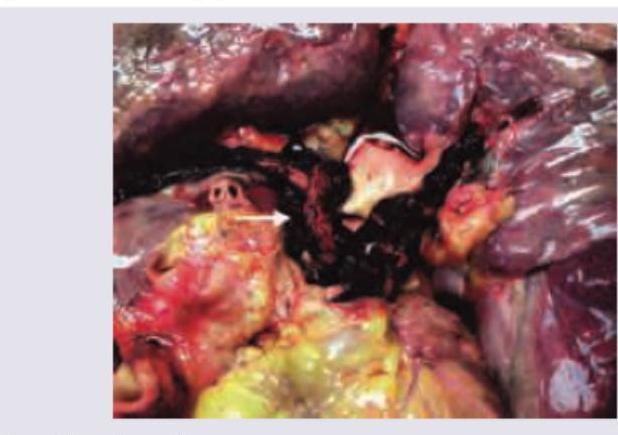
Postmortem lung specimen of a patient who developed severe respiratory distress and petechiae after fracture of shaft of femur is given below. All are true about the condition except:
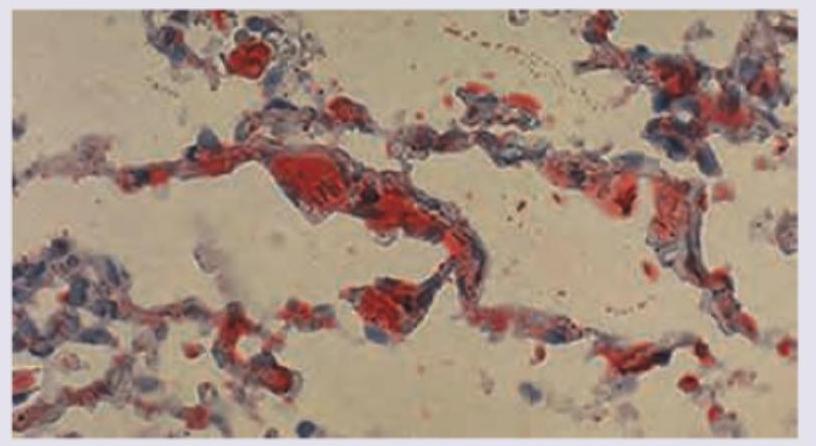
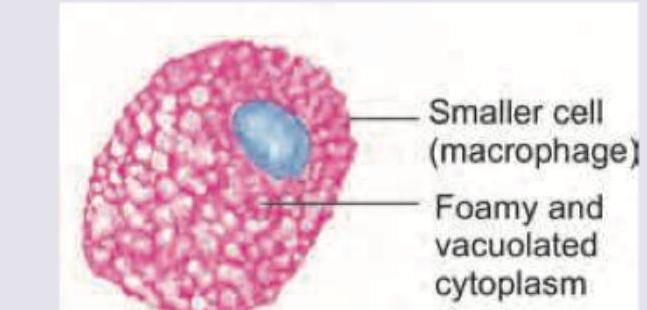
A 6-month-old child presents with loss of vision and regression of milestones. On examination hepatosplenomegaly and lymphadenopathy is seen. The bone marrow aspiration shows abnormal macrophage shown below. It stains positive for fat and negative for iron. Identify the cell.
A 50-year-old patient with family history positive for premature coronary artery disease is found to have lumps on Achilles tendon. Biopsy from the lesion shows presence of:
A 22-year-old biker had a road traffic accident with bilateral tibia fracture. After 7 days, his condition suddenly worsens and leads to death. Pathological specimen is provided. What could be the likely cause of death?
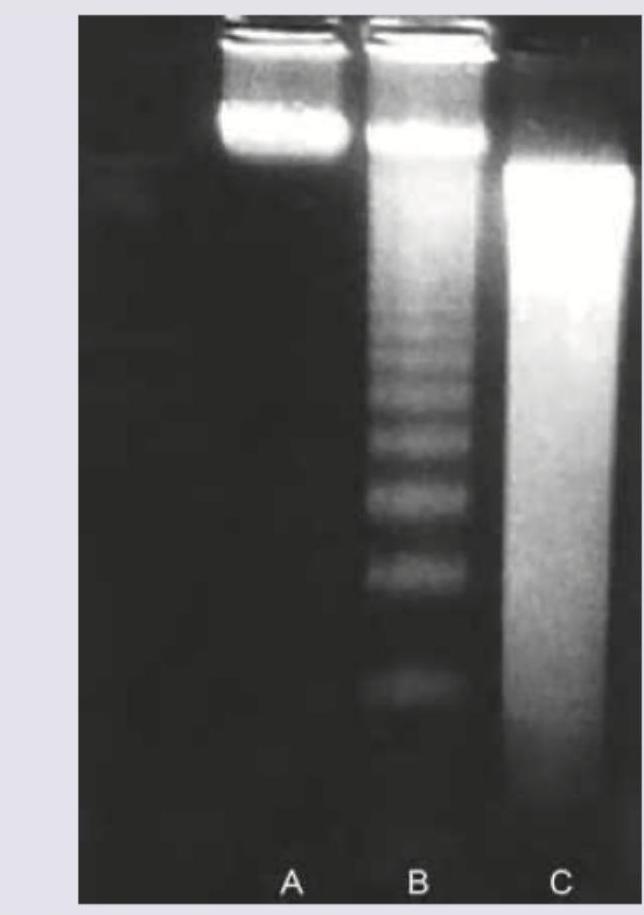
Agarose gel electrophoresis from DNA of a population of cells as seen under ultraviolet light is shown below. What is the correct explanation for the finding seen in the band labeled as "C"?
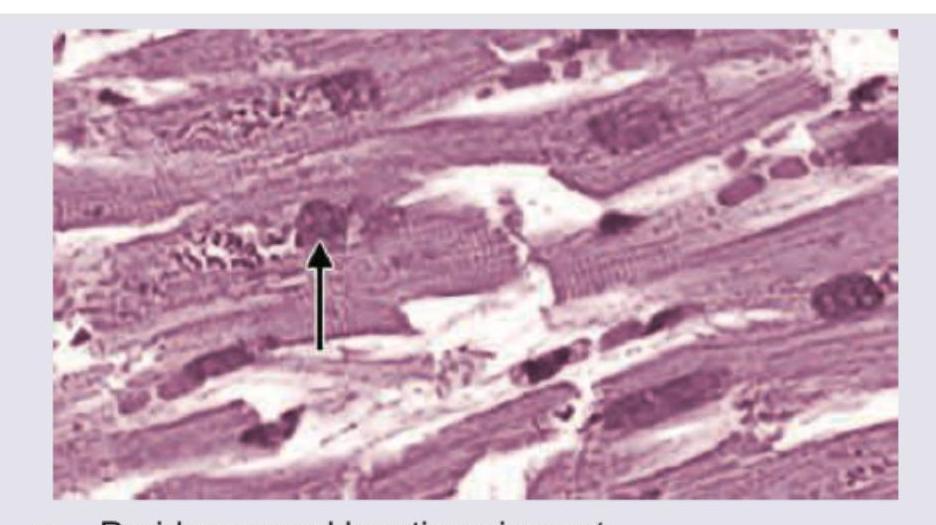
An 80-year-old Parkinsonism patient died due to pneumonia. All are true about the heart histopathology slide except:
Practice by Chapter
Cell Injury and Cell Death
Practice Questions
Adaptations of Cellular Growth
Practice Questions
Accumulations and Deposits
Practice Questions
Acute and Chronic Inflammation
Practice Questions
Tissue Repair and Wound Healing
Practice Questions
Hemodynamic Disorders
Practice Questions
Genetic Disorders
Practice Questions
Environmental Pathology
Practice Questions
Nutritional Diseases
Practice Questions
Molecular Basis of Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app