
General Pathology — MCQs

On this page
Necrosis with putrefaction is called as:
A study of aging shows that senescent cells have accumulated damage from toxic byproducts of metabolism, with increased intracellular lipofuscin deposition. Prolonged ingestion of which of the following substances is most likely to counteract this aging mechanism?
On electron microscopy, amyloid characteristically exhibits which of the following?
Which finding on electron microscopy indicates irreversible cell injury?
A 32-year-old woman with poorly controlled diabetes mellitus delivers a healthy boy at 38 weeks of gestation. As a result of maternal hyperglycemia during pregnancy, what morphologic response would be expected in the pancreatic islets of the neonate?
Intermediate filaments (IFs) help link adjacent sarcomeres together in skeletal muscle. Which of the following proteins is an intermediate filament protein used diagnostically in pathologic cases to indicate muscle origin?
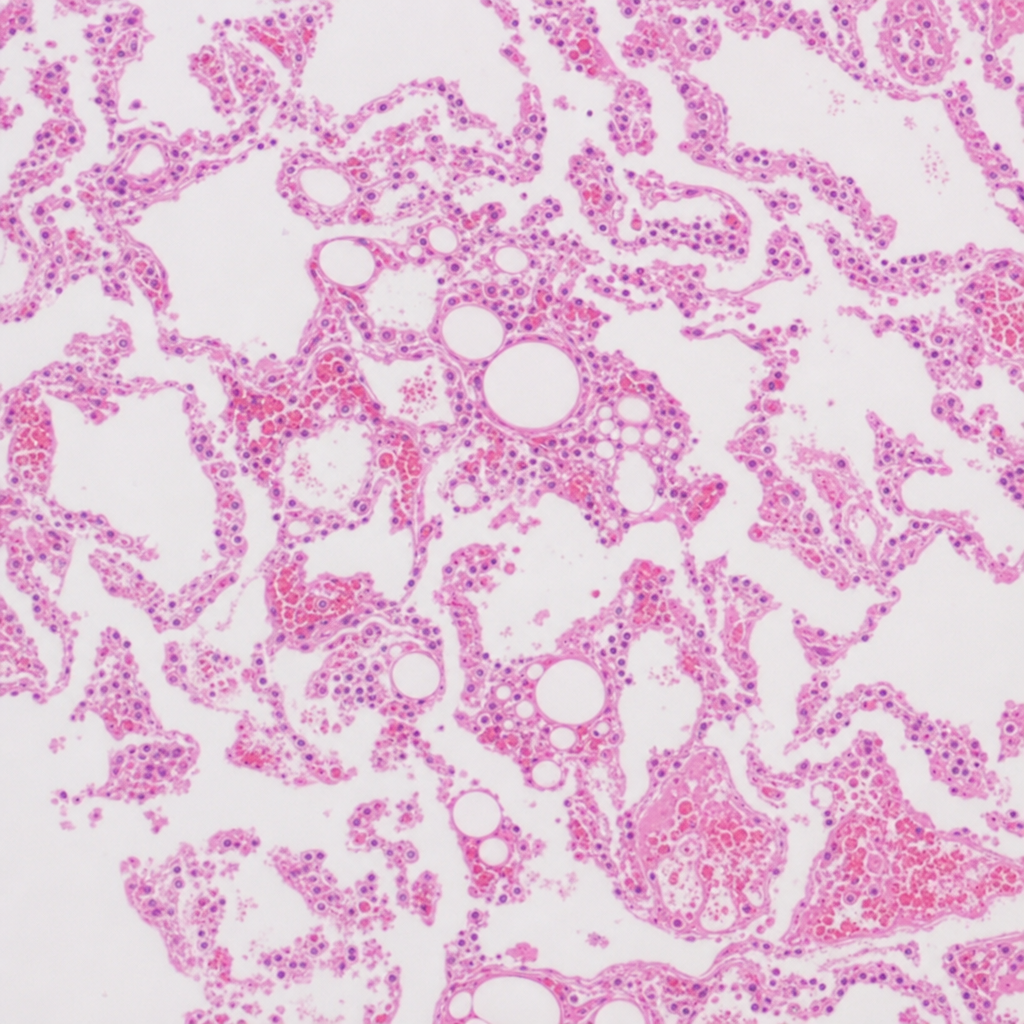
A 58-year-old man suffered a road traffic accident and came to the hospital. He had multiple fractures in his lower limbs, ribs, and lung contusion. Approximately 48 hours after admission, he developed progressive hypoxemia, neurological deterioration, and petechial rash over the chest and axillae. Ultimately, he succumbed to his injuries. At autopsy, a biopsy from the lung showed extensive fat globules in pulmonary capillaries. What is the likely cause of his death?
Which of the following is NOT a feature or common association of psammoma bodies?
All of the following are X-linked except?
A 22-year-old woman delivers an apparently healthy female infant after an uncomplicated pregnancy. By 4 years of age, the girl has progressive, severe neurologic deterioration. Physical examination shows marked hepatosplenomegaly. A bone marrow biopsy specimen shows numerous foamy vacuolated macrophages. Analysis of which of the following factors is most likely to aid in the diagnosis of this condition?
Practice by Chapter
Cell Injury and Cell Death
Practice Questions
Adaptations of Cellular Growth
Practice Questions
Accumulations and Deposits
Practice Questions
Acute and Chronic Inflammation
Practice Questions
Tissue Repair and Wound Healing
Practice Questions
Hemodynamic Disorders
Practice Questions
Genetic Disorders
Practice Questions
Environmental Pathology
Practice Questions
Nutritional Diseases
Practice Questions
Molecular Basis of Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app