
General Pathology — MCQs

On this page
All of the following are intermediate filaments except?
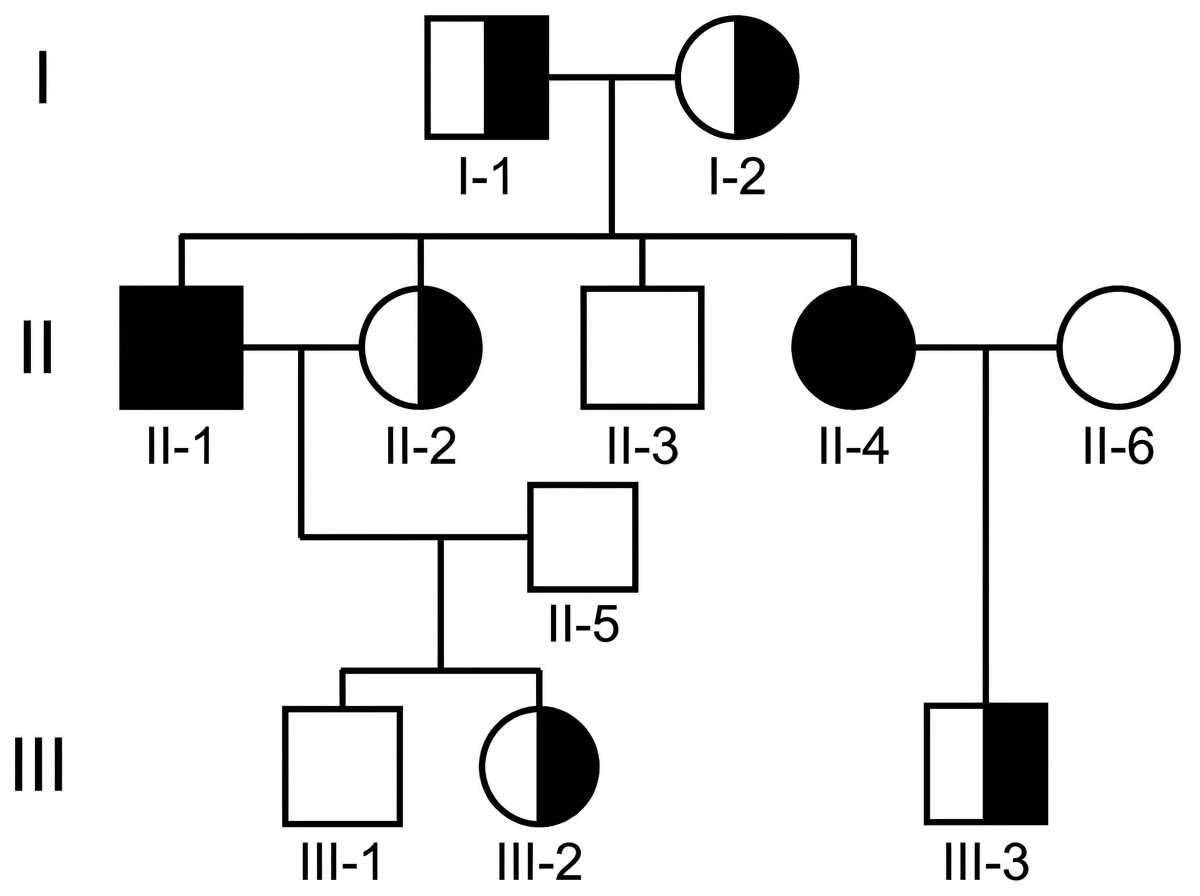
Examine the above pedigree chart. Which one of the following diseases is the most likely for this situation?
Which of the following is a proapoptotic marker?
Obstructive shock is due to which of the following mechanisms?
What is the most reliable investigation for amyloid disease?
Fat necrosis is classically seen in which organ?
Red infarction is typically seen in which organ?
A 4-year-old boy presents with extremely pliable skin, easy bruising, and joint hyperextensibility. Biochemical studies show a deficiency of lysyl hydroxylase. What cellular or tissue component abnormalities would most likely be revealed by ultrastructural examination of a skin biopsy from this patient?
Liquefactive necrosis on necrotic tissue results in which of the following?
Aspiration of fluid around the knee joint in a diabetic patient undergoing dialysis would show which of the following?
Practice by Chapter
Cell Injury and Cell Death
Practice Questions
Adaptations of Cellular Growth
Practice Questions
Accumulations and Deposits
Practice Questions
Acute and Chronic Inflammation
Practice Questions
Tissue Repair and Wound Healing
Practice Questions
Hemodynamic Disorders
Practice Questions
Genetic Disorders
Practice Questions
Environmental Pathology
Practice Questions
Nutritional Diseases
Practice Questions
Molecular Basis of Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app