
General Pathology — MCQs

On this page
Which stain is NOT used for lipids?
Aneuploidy is due to:
A CT scan of a 43-year-old woman with a parathyroid adenoma and hyperparathyroidism reveals extensive calcium deposits in the lungs and kidney parenchyma. These radiologic findings are best explained by which of the following mechanisms of disease?
Metaplasia occurs in all of the following except:
A 31-year-old man presents with infertility and aspermia. He reports chronic diarrhea with elevated quantitative stool fat, and has a history of recurrent, severe respiratory tract infections since early childhood. As a neonate, he experienced bowel obstruction due to meconium ileus. Which gene is most likely to harbor a mutation causing these symptoms?
Which organ is least affected by arterial thromboembolism?
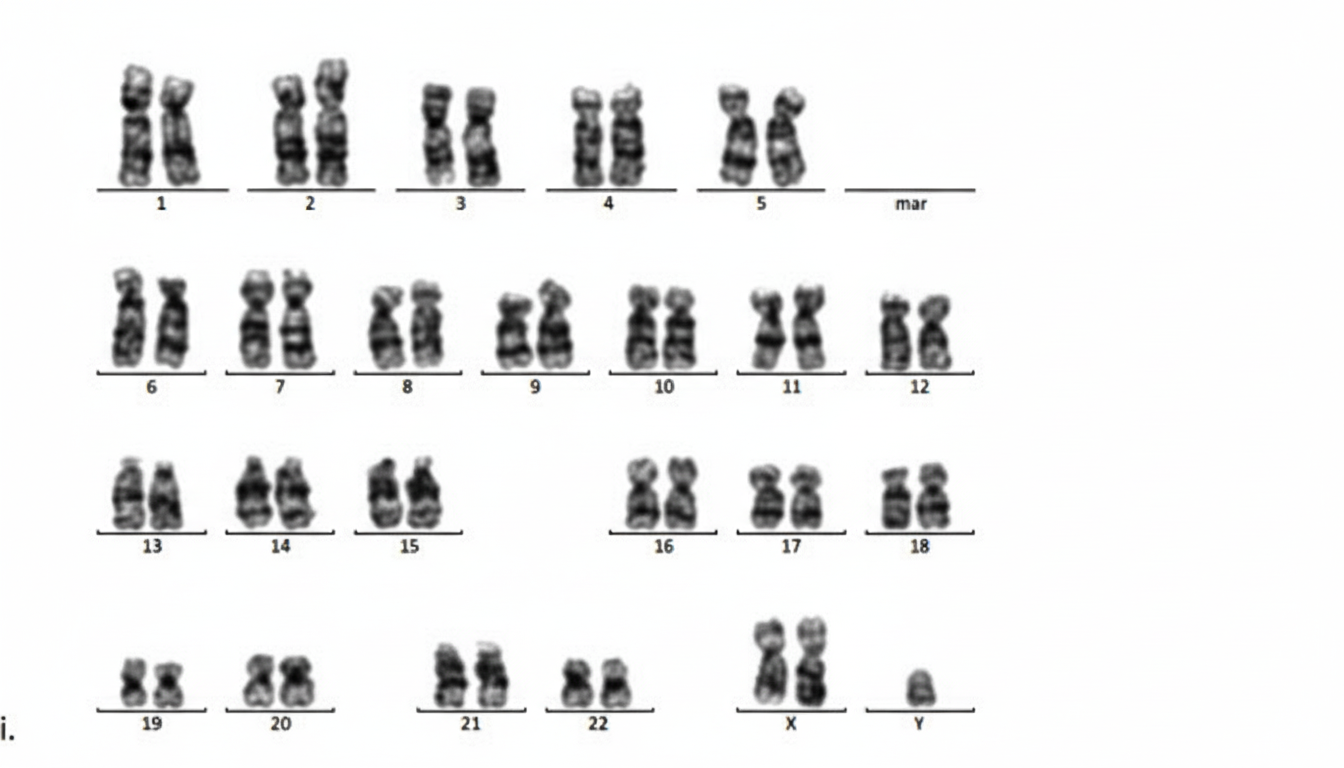
A married middle-aged female gives a history of repeated abortions for the past 5 years. The given below is a prenatal karyogram from one of her conceptions. This karyogram suggests which of the following?
In muscle hypertrophy, which myosin isoform changes?
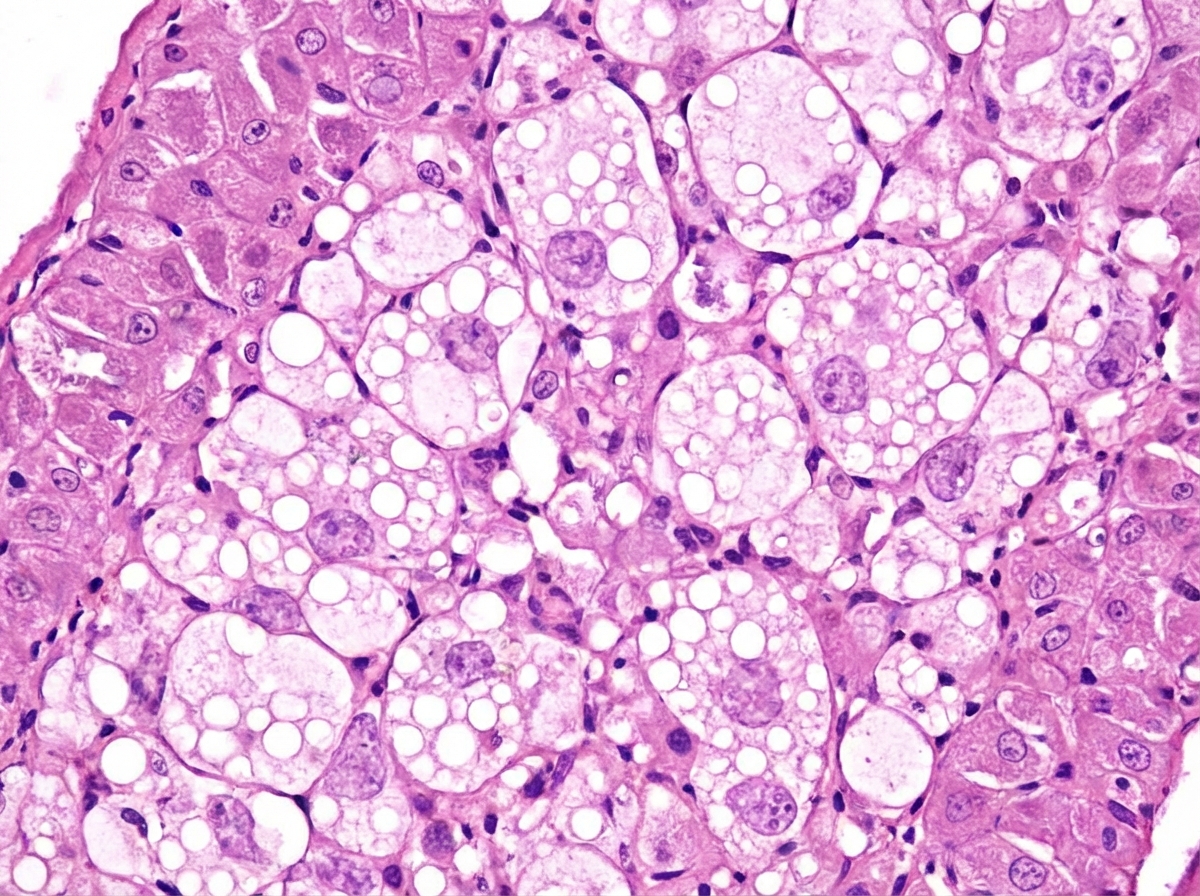
Which disease is characterized by the following histopathological finding?
A 60-year-old male patient complains of discoloration of his right leg. He is a known case of diabetes mellitus. Physical examination reveals blackish discoloration of the right leg with a dry and shrunken appearance. Which of the following most appropriately describes the condition of this patient?
Practice by Chapter
Cell Injury and Cell Death
Practice Questions
Adaptations of Cellular Growth
Practice Questions
Accumulations and Deposits
Practice Questions
Acute and Chronic Inflammation
Practice Questions
Tissue Repair and Wound Healing
Practice Questions
Hemodynamic Disorders
Practice Questions
Genetic Disorders
Practice Questions
Environmental Pathology
Practice Questions
Nutritional Diseases
Practice Questions
Molecular Basis of Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app